I taught university level courses in sociology and criminal justice for over 30 years but now I'm retired and at 72 was diagnosed with multiple myeloma, bone marrow cancer. This site is now a chronicle of my journey with myeloma.
I told you in my last post that I had gotten a skeletal CT scan a week ago Saturday, November 9th. I know what these scans are looking for and I was somewhat apprehensive about getting the results. I still haven’t heard from my oncologist about the scan and I won’t be talking to him about it until Wednesday, the 20th. However, my GP called me on Friday the 15th at 5:30 PM to talk to me. Truth is, whenever my GP calls at 5:30 on a Friday evening it’s never good news.
The first question he asks me is if I’d heard anything about the scan. I said no, nothing. He then proceeds to tell me that I have a four centimetre tumour (lesion) in my right femur. Now, that’s a fairly large lesion but it’s in a fairly large bone too. Still, one of the main problems with multiple myeloma is bone lesions. Patients can have several bone lesions simultaneously making their lives somewhat precarious. Any wrong move can lead to broken bones and immobility.
My GP is rightly concerned about this femoral lesion and tells me that I may need a full length splint to keep my leg immobilized but it’s Friday evening now and I’m in no shape to even consider getting one, especially if it means going to the ER. That’s not going to happen. Not in a hundred years!
After a time my GP and I settle on a plan to keep me more or less immobilized, at least until Monday. Carolyn and I get back to our dinner. A while later my GP calls again after having consulted with an orthopaedic surgeon. The surgeon tells him that I will probably need radiation on that tumour and that radiation treatments happen in Victoria. Until then, I need to keep my right leg as immobile as possible. We’re getting a wheelchair on Tuesday. That will help, and on Wednesday I talk to my oncologist about where we go from here in terms of chemotherapy and now radiation treatments.
You know what? I want some straight answers. That’s all. I know that straight answers are not as easy to come by as they should be, but I’d like a clear, unadulterated assessment of my prognosis at the moment, if you don’t mind. So far, my oncologist and I had not even discussed bone lesions and the treatments for them, and we assumed that the lenalidomide/dexamorphosone chemotherapy drug combination would work and that we would reassess in a year or so.
Yes, I understand that multiple myeloma is highly treatable although it’s incurable, but every myeloma patient presents with an idiopathic set of conditions making blanket prognostications about remissions and potential lifespans kind of useless, if not overly optimistic. So far I have no idea how bad a case of myeloma I presented with and my oncologist is not really interested in what stage I’m at. He says he’s much more interested in how a patient responds to treatments than where they might be on a staging continuum. That’s fine. I hope that sometime soon we will actually be able to assess just how I’m doing on a new course of chemotherapy drugs and that we will be able to conclude that what I’ve experienced so far is a temporary glitch in my treatment.
Whatever. I like taking road trips on winding roads in unfamiliar territory, but a nice stretch of open highway now and again can be exhilarating too. I’d like to see some open road for a change where obstacles can be seen a long way off and I can put the petal to the metal. Is that too much to ask for?
[A note: I’m used to writing posts here of approximately a thousand words. Because I’m so fatigued with anemia and other conditions that affect my concentration, for the foreseeable future I’ll make my blog posts a little shorter. That way I will be able to continue writing and not tire myself out too much.]
I started the chemotherapy drugs, lenalidomide and dexamethasone last Thursday morning. I was to take one lenalidomide tablet and five dexamethasone, continue with the lenalidomide for three more weeks and five dexamethasone tablets every Thursday morning until they were done. Frankly, it was a relief to finally get going on a treatment for my multiple myeloma (MM), any treatment. Well, you know what they say about the best laid plans of mice and me. They never go according to plan, and this was not about to become an exception to the rule.
It must have been Saturday (I got a CT scan that day) when I noticed that my butt was getting really itchy. Well, naturally, I scratched it. I knew it isn’t a good thing to scratch an itch, but I just couldn’t help myself. The welts just got bigger and hotter and covered my whole midsection. I developed a slight fever. Carolyn, my very competent care aide spread some lotion on my backside and up under my armpits to relieve some of the itching. Damn good thing too because I was close to losing it.
Well, it turns out that the reason I developed this rash in the first place is that I happen to be allergic to my main chemotherapy drug, lenalidomide. Now, that’s not cool! Lenalidomide is an oral therapy drug, and for that reason is very convenient to take. So, it’s the weekend, I’m itchy as hell, but I persist in taking my chemo meds. On Tuesday, yesterday, I call the oncology nurse in Victoria who seemed quite concerned about the rash. She tells me that she would try to track down my oncologist to get some idea of what to do. My regular oncologist was out of the Cancer Centre at meetings but she tracked down his colleague who told the nurse to tell me to cease taking lenolidomide immediately. So, great. Here I am, not a week into taking my first course of chemo meds and now I can’t take them anymore! What the hell is that all about, universe?
I was pretty bummed out for a time there, but then I realized that this is not an uncommon turn of events in oncology. In fact, about 40% of people enrolled in the lenalidomide/dexamethasone regimen turn out not to be able to tolerate the drugs.
A Cancer Clinic receptionist called this morning to set up a telephone consultation with my oncologist for the 20th, next Wednesday. At that time I should learn more about my next course of treatment as well as what they learned from my last CT scan. Strangely enough, I also got a call from the hospital here in Courtenay telling my that I needed to call them and set up a second course of treatment. She mentioned lenalidomide and I said it’s unlikely that it would be for lenalidomide because in all likelihood, I’m allergic to it and I was told to stop taking it. I guess it takes a while for messages to get from Victoria to Courtenay and back. I soon learned to take all phone calls from the hospital or the Cancer Clinic with a grain of salt and usually wait for confirmation from a third source before moving on with anything.
In my next post I’ll address the fun topics of pain, hallucinations, and cold sweats.
I was going to write a post about the social triage that happens in emergency departments everywhere, and I will get around to that, but for now I have other more pressing issues to deal with. I’m intent on documenting my experiences with myeloma as completely as possible so, for the moment, that will be my priority for this blog. One strange thing that’s happened to me is that I have a recurring dream about the emergency department at the Royal Jubilee Hospital. More on that to come.
Before I do that, however, I want you all to feel free to contact me. If you have problems with privacy i.e., you don’t want your comments to appear in public, please let me know when you post comments, or pm me on Messenger or you can email me at rogalb@shaw.ca.
Things can change very quickly these days and positive things do happen! Oh, I still have myeloma and I started chemo yesterday. That seems fine. The pain in my neck has attenuated too. Who knows why. I can feel it lurking around my cervical spine, but for now it’s keeping a respectful distance. I can actually type and stay relatively focussed. I pay for that by not taking as much hydromorphone. AND my kidney is back to normal…for an old guy like me anyway and that’s very good news. I was thinking I may need a wheelchair to get around and we were making arrangements for that, but for the moment, I’m good. I’m feeling okay at the moment, ten times better than I felt two days ago, but that’s how it goes with chronic pain. Things can easily go back to shitty in a flash. Of course I know that I’m an old guy with cancer and I can see the exit door over there just beyond the bright white light, but I can’t see the handle yet, so I think I have some time. Besides, I can put that to the back of my mind. It doesn’t help at all to focus on things I can’t inevitably change and stick to the things that can get me, and others, better quality of life now and for the near future.
So, pain. My last blog post was about Carolyn’s experiences at the Emergency Department here in Courtenay. My penultimate posts were about my visit to the oncologist in Victoria and my subsequent disastrous ER visit the following day. I sit here somewhat unable to piece together accurately in sequence what happened to me since last Wednesday. Truth is I’ve seen two specialists since then, have had a ct scan with another one scheduled for tomorrow which showed that I have severe disk degeneration in my neck that is, along with arthritis, creating the pain vortex in my neck. My neck pain has been a roller coaster of severity. I have a neck brace that helps with that too as you can see from the photo below. Hi!
My office
Now, this is where it gets interesting because my oncologist tells me that my neck pain has nothing to do with my myeloma. It has everything to do with my disk degeneration and arthritis. So, I ask: does the myeloma contribute at all to pain in my body? Of course it does, comes the answer. It attacks your bones. The ct scan did not find the right kinds of lesions on my cervical spine, so they were not the source of my neck pain. Well, okay. I guess I can go along with the argument that my nasty bulging disks are responsible. I mean I had surgery on my lower back decades ago to alleviate a ruptured disk problem so I’m familiar with that. Still, recently I’ve had over the top thoracic skeletal pain which really was caused by my myeloma so whatever. I’m getting a ct scan tomorrow to check that out among other things.
So, what I’ve been able to piece together through moments of excruciating pain and hallucinating sedation, is that the pain I’m experiencing the most severely seems to be concentrated in the bony/connective parts of my body that had already suffered trauma. I’m thinking specifically of the area on my left thorax where my kidney as removed, the lower back cervical area where I had a disk removed, the left heel where I had planers fasciitis, that sort of thing. My neck too and my shoulders where I had rotator cuff tears, both sides due to falls and long term overuse issues.
I started asking this question to whoever would listen: is there an association between myeloma and increased intensity of pain in areas of previous bone trauma? Answer: I don’t think so, but probably not. Question: Do you know of any research between myeloma and where it affects the body most? Answer: Not that I know of. I had a chat with my daughters about this. They’re no slouches when it comes to research: One of them works in the field of non-profit housing and the other in biomedical research. They are my truly trusted experts. But, I have access to a lot of material too because I’m still associated with North Island College as emeritus and have library privileges.
Okay, that still leaves me dealing with my own experience of pain and those of others (read the comment by Tanya Wood based on my last post), some of whom have chosen to remain anonymous. I’m especially concerned with Emergency Departments and with receptionists (gatekeepers) in GP offices who, I know are just doing their jobs, but who, when I call to simply ask that can the doctor just tell me if I can increase my dosage of hydromorphone says: “Well, the doctor will have to see you for that” To which I answer: I can barely move. I have excruciating pain and can barely get out of my chair. Can he just tell me quickly about increasing my already existing prescription with pills I already have?” “Well, no, the doctor will have to see you.” So, I couldn’t take anymore of that and told her we’d get back to them. Later, Carolyn called and talked to someone else who said someone would be in touch. My doctor called me later in the day when he had done his patient visits for the day, something he as often done in the past and I knew he would do again. So, all day I was left figuring out how many more hydromorphone pills to take before overdosing. I’m not at all suicidal, so that’s a concern. I’ve known of many people who have died from accidental overdoses. I wasn’t about to be one of them, but my pain was so intense it was a good thing I wasn’t standing at a subway station waiting for a train anytime last week. I may just have acted compulsively and jumped onto the tracks. Of course that’s a little hyperbole, but that’s okay among friends, isn’t it?
I wrote to Tanya Wood (who’s husband, Darren, died a couple of years from complications resulting from a tragic accident) in response to her heart wrenching comment that ER departments are microcosms of our culture. They operate using the same moral assumptions as everyone else in society. We have deep-seating cultural aversions to death and disease. Most of those are built on our huge biological insecurities. I paraphrase here Ernest Becker who wrote something like: Disease takes away our ability to enjoy the pleasures of life and death does that permanently. He calls death and disease the twin pillars of evil for us. [You need to read some of my early posts to get a sense of how brilliant I feel Becker was.]
So, in a sense, I’m not surprised at the cavalier attitude most staff members have towards people coming into Emergency departments everywhere. Don’t get me wrong. There are some very dedicated and caring medical staff working in ERs doing a mostly thankless job which, I’m sure, can be extremely rewarding at times too but the system is stacked against them and they will, I’m certain, be looking for different work soon if they don’t toe the line. And, of course, as I’ve already noted in a previous post that pain is invisible so ER staff can’t just take your word for it. Not only that, but if you come in really agitated that you’re in extreme pain and need some meds now they may tag you as a troublemaker and make you wait all that much longer for help. There’s a big screen tv in the ER waiting room at the Royal Jubilee Hospital explaining in great detail why you must wait and why. There are signs saying no foul language or threats or whatever will be tolerated. There are security people everywhere dressed just like police. I wonder what they would do if somebody with Turette’s Syndrome came in following a car crash or, as is quite common, some people can’t utter a full sentence without ‘fuck’ in it at least once. These people may just suffer from undeveloped communicative skills but they are probably not dangerous. The message is clear: if you want treatment here you had better stay calm, cool, and collected. Of course, precautions must be taken, but I’m not sure that blanket prohibitions are the way to do it.
Pain, in our culture, is associated with weakness and most people are loathe to talk about it even to the point of not seeing a doctor because they’re embarrassed about the location of their pain or don’t want to admit weakness. Weakness of any kind is just not acceptable. Do you see any weak superheroes in the movies? Well, some of them show some slight or passing weaknesses but they always triumph over them in the glorious light of their super strength. That’s in the movies. In Diehard movies the hero falls off of an eighteen storey building onto the top of a moving van below, rolls of of that onto the sidewalk where he encounters villains walking towards him shooting up a storm with their AR-15s (or whatever), gets hit, falls through the open door of a bar, sidles up to the bartender and asks for a scotch on the rocks. The young, gorgeous, female bartender gives him his drink and comments on the two gaping bullet wounds on his shoulder. He respond in true superhero in training fashion: “These, nah, just flesh wounds.”
Real heroes are immune to pain it seems so if you really want to be a superhero, boys and girls, don’t complain about pain!
Pain doesn’t kill. It’s a sign that something organic is out of whack and needs attention. Failure to attend to pain often results in dire consequences for the patient but any complaint of pain is not treated initially by medical staff as an organic issue, but rather as a moral one. We are all assumed to be moral degenerates unless proven otherwise by the cognoscenti. Of course that’s not true in every case, but the underlying assumptions are always there. Overlying all of this too is the assumption that there is an acceptable amount of demonstration allowed with different levels of injury. So, for a broken leg, some amount of whimpering is allowed, and for the pain I went in with some moaning and groaning is okay, but only when there’s movement happening otherwise sitting quietly is what’s expected. In any case they have a scale of acceptable pain demonstration. Don’t mess up their expectations and assumptions. But as I said, our reaction to pain culturally is really screwed up so you’d have to think that in an ER that would be doubly evident. It’s not right but that’s the way it is. Is there anything we can do about it? Maybe, but it’s complicated and requires a lot of knowledge and challenges to authority. Authority does not like being challenged. That itself is a challenge since authority has all the lawyers it wants to line up against you, often using your money. But lets poke the beast a little and see if it demonstrate any signs of weakness or pain.
I’m not dead yet, and I’m coming for you, VIHA, and related government departments and agencies. You’re trying to get rid of pathology services entirely in the North Island and that’s a travesty. Some of you in the business may need to retake your Hippocratic oath. More on this later. I need to do more research to know exactly what the situation is, but when I’m ready you’ll know about it.
So, for now, I’ve seen my oncologist, my kidney specialist, my pathologist and now I need to have my beer specialist on my team. I won’t be going out to see him anytime soon, but I heard he might just deliver. Damn, there’s so much more to say!
One of my previous posts about disability and people in wheelchairs. It might be of interest after reading this post.
Well, giddy might not be exactly the correct word to use here but it’s close. I’ve known for a month or so now that I have multiple myeloma, an incurable bone marrow cancer, but I have also been told that it’s treatable and some people live for some years after their diagnosis. But I’m not sure about anything yet because I have yet to see an oncologist. That changed yesterday, at least the anticipation part.
Yesterday, around 1 PM I got a call from the BC Cancer Agency in Victoria, telling me that I have an appointment with an oncologist at the clinic on Thursday, the 31st of October, Halloween morning, at 10:30 AM. I have no idea what to expect because I have no idea at what stage my cancer is at nor what treatment options there are. Oh, I can make up stories based on Dr. Google research, but that’s a futile pursuit. This disease is idiopathic. No two patients are alike. I guess that’s true for most cancers. There are commonalities and there are individualities. The only reason they can be treated at all is because of the commonalities. Without pathological patterns no illness could be treated. Still, the idiopathic aspects of this disease make it hard to compare experiences with others facing the same disease. We can commiserate, but that’s about as far as it goes. That said, there is comfort in commiseration.
So, this morning at 7:45 I attended the medical lab in Cumberland so they could take a dozen vials of blood and some urine (boy, did I have to pee when I got there) in anticipation of my appointment with the oncologist, but also with a nephrologist in Nanaimo on November 7th. On Saturday I have a CT scan and on Sunday I do a twenty-four hour urine collection for the nephrologist. I might already have told you this, but I am taking prednisone now and I’ve had an infusion of some drug the name of which I forget. So, in effect, my treatment has already started. I can’t wait to see what the oncologist has in store for me come Halloween morning.
I’m always a sociologist so whatever happens to me triggers an instinct I have to do check it out, do the research, connect the dots. In my book, the more information we have the better. At the moment, we have an information deficit and that’s frustrating but, hopefully, that’s about to change.
In any case, one of my first research stops is Statistics Canada. What’s there to learn there? Well, for one thing, multiple myeloma (MM) is a pretty rare form of cancer and that makes me special, don’t you think? Stats Can reports that there will be about 3000 people in Canada diagnosed this year with it. That’s not a very high number. Stats Can also projects that from 2018 to 2022 only 70 men in BC will be diagnosed with MM in my age group every year. Because doctors seldom encounter it, it can be difficult to diagnose, but back to that in a bit.
I’m in good company too when it comes to MM. Jim Carr, the Liberal Member of Parliament for Winnipeg Centre and Minister of International Trade in the Federal Cabinet, was diagnosed with MM the day of the election (Monday, Oct. 21st) when he went into the hospital complaining of flu-like symptoms. By Tuesday he was receiving chemotherapy and dialysis and by Thursday the CBC was reporting that the Minister said he was doing fine, felt okay and was going to continue serving his constituents and the Canadian People. I’m so happy for him. He won’t be cured, but he will probably be able to function quite well for some time to come. By contrast, my doctors knew I had MM three weeks ago and I have yet to see an oncologist and will have to drive 225 kilometres to Victoria for the pleasure. Living in the boonies as we do, access to specialized health care can be spotty at best and will only get worse if the Vancouver Health Authority has its way. (That’s the subject of another blog post but DecafNation, George Le Masurier’s excellent blog, has been on to this for some time). It’s true that an oncologist in Victoria is on my case and has already prescribed medications for me and I got an infusion of a drug a couple of days ago at the hospital here to help with the pain and ‘strengthen bone’. Still, I feel that I’m not getting the level of care I would have gotten if I were a member of the Canadian political aristocracy or if I lived in a large metropolitan centre. My age likely has something to do with it too. I’m an old guy and not likely to live too long anyway and besides, I’m no longer a contributing member of the economy having retired from teaching at North Island College in 2012. Does that sound like sour grapes? It may be, but socio-economic status (class, gender, age, and geographical location, etc.) has a lot to do with health care provision whether we like to admit it or not.
Alright, so back to my situation. I’ve probably had MM for a long time. I have low B12 and was diagnosed with pernicious anemia at one time by a locum (temporary replacement for my regular doctor) , but my doctor didn’t really accept this diagnosis and prescribed B12 monthly injections (which I do myself). The thing is, I had been going to my doctor for years complaining of being tired, having brain fog, being in lots of pain, and suffering from peripheral neuropathy. To give my doctor credit, he ordered MRIs of my brain and spinal cord, lower back, ultrasounds, etc., because there is a history of Multiple Sclerosis and other immunological diseases in my family. To add to this, I has a kidney removed in 2002 because of renal cell cancer, leaving me with one kidney. For a long time we tested my creatinine levels to ensure my kidney was functioning properly and it did for years. In the last three or four years however my kidney showed signs of being very unhappy. Creatinine levels were rising and still are, and I was getting weaker and weaker all the time with worsening symptoms.
My social life was taking a huge hit. Over the past few years I’ve had to pretty much give up going out in the evening because I’m exhausted. I had to give up life drawing, printmaking and sculpting. I had to resign from the Village of Cumberland’s Homelessness and Affordable Housing Committee and I had to resign as Chair of the Board of the Comox Valley Art Gallery (although frankly I had been doing that long enough). I can no longer go on long walks with Carolyn, something that we both really enjoyed.
After a while, I think my doctor kind of gave up trying to figure out what was wrong with me and I was beginning to wonder if it was all in my head.
About a month ago, all that changed. We had gone camping in Strathcona Park in August. I was not feeling great, but well enough to get the canoe out and paddle/sail/motor around a bit. A couple of times, however, we got into bucking huge headwinds and were forced to paddle hard. Carolyn and I are seasoned paddlers and we know what to do. I felt pretty strong and we handled it fine. Of course we had some muscle pain, but scotch helped out with that a bit! Then my daughter and her family joined us. One day as I was sitting at the camp site doing nothing, my back started hurting something awful. By the time I decided to take some ibuprofen (not to be taken by anyone with any kidney issues) my pain was pushing 9 or 9.5 on a 10 point scale. I was taking T3s like they were candy. When it was time to go home, my son-in-law drove the truck and trailer. I rode shotgun. I have driven very little since and not at all for the last month.
A short time later, I made an appointment to see my doctor to let him know about the back pain and my use of ibuprofen. He figured we had better do some blood testing and we did. He was headed out on vacation for three weeks so I wouldn’t be seeing him again until Oct. 22nd or so. Well, he called me on Friday at around 5:30 and told me that my kidney was leaking protein into my urine and that he had referred me to a kidney specialist in Nanaimo. That was a bit of a shock. I didn’t quite know what to say so I left it at that.
Over the weekend, Carolyn and I sat down and wrote down all of my symptoms and questions to which we wanted answers. On Monday, I called the medical clinic and got an appointment to see a locum to ask questions about what a protein leak meant and to lay out my symptoms. Well, he ordered more blood tests and imaging. We saw him again on Thursday by which time he already had a strong suspicion that I had multiple myeloma. On Friday he called and pretty much confirmed the diagnosis. On Monday we saw another locum and she ordered more tests and imaging as well as a bone marrow biopsy. She also referred me to the Cancer Clinic in Victoria.
So, in less than ten days, the locums had figured out that I had cancer and were moving fast to get me treatment. Possibly all that it took was a fresh set of eyes on my case. Certainly, the referral to the kidney specialist would have got me some results but I’m not scheduled to see him before November 7th. I wondered what my regular doctor would say when he got back from vacation. I am definitely pissed off that I went so long undiagnosed, but I don’t really blame my GP entirely for that. I may not have impressed on him the real state of my distress and MM is not easy to diagnose because it shares symptoms with so may other ailments. Besides, raving about past injustices will get me nowhere. I need to focus my full attention on the present and the future.
So, in any case and in the meantime, I called the Cancer Clinic and a person there confirmed my referral, gave me an ID number and said that I would be seeing such-and-such a doctor. Well, my regular doctor informed me just this past week that there had been a mix-up in the referral and that I would be seeing another doctor at the clinic. We have yet to hear from the Cancer Clinic. If I don’t hear from them by tomorrow afternoon I’ll be calling them again. We need some goddamn answers and I need to get some goddamn treatment. Stay tuned.
I’m sitting here pretty much incapacitated by some undetermined health issues, anticipating yet another doctor’s appointment tomorrow to go over yet another set of lab results, and trying to distract myself from too much inward looking self-pity. At least I can still write. The brain fog I’m experiencing makes it somewhat more difficult than in the past, but I can still do it, especially if I write about something I have some passing knowledge of.
A new American Civil War? Perhaps. The first American Civil War in the 1860s was fought by agricultural capitalists in the South against industrial capitalists in the North but it was couched in state-based rhetoric: Northern states versus Southern states. During the war, there was less emphasis on the economic interests than on slavery, ‘freedom’, and the need for a ‘United’ States. Capitalism can tolerate slavery to some extent, but it really needs a labour force that is also a consumer force. Slavery is incompatible with a growing need for mass consumption. Of course the first American Civil War was fought using non-economic rhetoric and propaganda but the underlying logic of the war was economic and political. Contemporary Confederate flag wavers are not focussed on economic, but on some imagined lost ‘freedom’, and Southern solidarity: Us hard-done-by-Southerners versus You overbearing, holier-than-thou Northerners. The longevity and sustainability of Southern feelings of oppression by the North should tell us something about the depth of feeling in the US now. Looking at a map of the US featuring red and blue states illustrates that there are still glaring geographical differences in people’s attitudes and in their political loyalties. The Southern states, now including Texas, are still feeling hard-done-by. (Some of the northern mid-American agricultural/rural states likewise). Visiting Texas it’s clear that there is an underlying uneasiness and separatist impulses have not completely dissolved. I haven’t visited Idaho, Wyoming or Montana, but rural, agricultural areas are clearly alienated from New York and California. It may be the United States of America, but it’s not the Solidarity States of America. Internecine squabbles and jealousies abound.
The Second American Civil War may well have a rhetorical veneer of statism and rage (yes, rage) over perceived (and sometimes real) social and economic inequalities, but if Donald Trump is successful, it will be a moral war, one fought by people who have fully absorbed the moral imperatives of the capitalist promise of free enterprise (while hardly benefitting from it personally) against people they perceive to have abandoned American ‘freedom’ and ‘liberty’. The move to impeach Trump will only further solidify the camps, but Trump has not given the Democrats many options. I’ve recently read a number of articles in the New Republic and in other publications that argue that the way to combat Trumpism is not to call out Trump supporters as stupid, ignorant morons, but to engage in dialogue and community building with them so as to understand their grievances and support them in coming to a more reasoned assessment of the issues. I’m not sure there’s time for that.
Trump will continue to inflame passions with his frequent Tweet storms and rallies, accusing high level policy makers of treason and high crimes. How long can this go on? How long will it be before we see a convoy of Mad Max wannabes rampaging through the streets of America’s major cities randomly shooting people, raping and pillaging? How long will it be after the initial skirmishes and outburst will be see anti-Trump militias grow in defence of their families and communities? What of the police? Will they serve the American Constitution against concerted attacks on democracy from all sides? Will they be peacemakers or will they take sides? And what of the military? Will the military take sides? Would the military support Trump if he decided not to vacate the White House after a narrow electoral defeat in 2020?
It’s dreadful to even think about possible scenarios of violence, lawlessness, and totalitarianism but to not think about them is irresponsible.
I’m a Canadian. As Pierre Trudeau said decades ago, we are a mouse sleeping next to an elephant. Woe be the moment when the elephant rolls over in his sleep. For Canadians there is no isolation from American extremism. Over 80% of us live within a hundred miles of the American border. We have family and friends in the US. We worry about their safety and security.
I am a retired college teacher. I told my students decades ago that America was headed for a civil war. The tensions caused by American corporations creating global markets and (at least for the moment) eliminating good paying jobs in manufacturing to exploit cheap labour in Asia, Africa and South and Central America, were bound to lead to widespread social unrest, nationalism and jingoism. I don’t think that global supply chains and markets are going to be easily dissuaded by Trump. They continue to create subsidiaries and engage contractors in China, India and elsewhere. North American manufacturers continue to expand their supply chains and are not interested in containing their activities to US territory nor would they be interested in repatriating manufacturing. I can’t imagine Nike returning to Oregon to manufacture its products. It has no capacity to do so in the US and it would be prohibitively expensive to build new factories in Beaverton, Oregon, the site of its headquarters. There are some agricultural corporations that are moving their processing facilities from Canada to the US in a move, in part, to placate Trump supporters, but they still need Canadian raw materials. The complexity of global capitalism is staggering and strangely enough, that is what gives me any hope at all that a second American Civil War can be avoided. Many US manufacturing corporations that keep research and development functions in the US but produce their commodities everywhere else on the globe are pushing back against Trump’s tariffs. For example, iPhones are made in several places, mostly in China (check out FoxxCon) but may also be made in India shortly. US tariffs will force the price of iPhones upwards, but that’s true for many so-called American products made in China and elsewhere. The world is now so economically intertwined and interconnected that starting a war with China, say, means crushing America’s own manufacturing and processing capacity. I’m hoping that America’s business leaders will have the guts to seriously oppose Trump. I’m not sure that will happen and they may just try to wait him out. I’m unconvinced, however, that any business opposition to Trump will be able to coalesce sufficiently to help ease tensions in the US domestically.
The picture is much more complex than I’ve presented it here, and I may be a victim, like many others, of hyped up, sensationalist news. However, I perceived, like others, this trend in America for decades, before social media, fake news and the gutting of the CBC and other formerly independent news sources. I read widely and I search out different points of view. Trump supporters are caught up in a cult-like mindset unencumbered by reason and will not easily be dissuaded even if dire predictions of the imminent collapse of America do not come to pass. Sadly, some extreme lefties are caught up in the idea that all Trump supporters are ignorant, stupid slobs. There isn’t much room for moderation, reconciliation, or peace in this extremism. Is it possible for the political ‘middle’ to assert itself and put a stop to all forms of extremism? If so, how would that happen? If not, where do we go from here?
So, I’ve had chronic pain for decades, at least since the early 1990s. I use acetaminophen regularly, sometimes resorting to T3s and even hydromorphone (oral morphine) on occasions where the pain and discomfort were (are) extreme. I can’t take ibuprofen because I have only one kidney (my left one was removed because of cancer in 2002) although it works the best for me. The other day, as a tribute to our silliness, Carolyn and I went canoeing on Buttle Lake in Strathcona Park. Such a beautiful place, but the wind can come up very strongly. We knew it could do that, but we blithely went out in the canoe anyway, and surely enough we got caught in a very snotty windstorm. We had to paddle at ramming speed for quite a while. My 72 year old body protested on every stroke. A couple of days later things came to a head and I had excruciating pain in my back because of a severe muscle strain (probably a tear, but who’s quibbling). So now I had acute pain competing with my chronic pain for attention. Both were winning at this stage. Enter CBD and THC.
There are lots of websites extolling the virtues of CBD and THC for the treatment of chronic pain, arthritis included. Here is one example from Medical News Today. WebMD is what I judge to be a fairly reliable source of internet-based medical information. Like this article in WebMD argues, consulting a physician is always important before using CBD as a medicine.
Great, so in the interests of attempting to alleviate some of my chronic pain, and being desperate, I decided to try using CBD and THC. To that end I had an MD ( a locum in my medical clinic) refer me to a group of health care professionals (physicians, nurses and therapists) at a clinic not far from my home. I figured I’d be a test subject although I know very well that a one person study is not a study at all. I was called shortly thereafter to a consultation with a physician who has experience with using CBD and THC medicinally. I was prescribed the use of CBD daily for chronic pain and THC at night to help me sleep through the night. On the physician’s recommendation I bought a 40 MG vial of CBD and a 40 MG vial of THC from what they said was a reputable manufacturer. So far, I’ve found that the manufacturer has been very careful to sell me only what I have a prescription for. The physician I saw prepared for me a sheet of instructions for taking CBD and THC. Since then, I’ve had regular calls from the clinic inquiring as to my experience with the products. I completed my first course of using CBD and THC a while back and have recently picked up my second prescription.
I really hoped that CBD and THC would work for me. T3s are fine, but harsh on the stomach. The THC is fine. It gets me stoned to some extent so I tried to take it only at nighttime. Doing what I do in my daily life, I can’t be stoned all the time. I need a clear(ish) head. I have enough trouble with brain fog as it is because of my immune disease. I don’t want to add to it with meds that don’t work all that well. I don’t think CBD worked for me at all, ever. I kept giving it a shot paying very close attention to my symptoms but I felt no improvement.
After I injured myself canoeing, I saw an MD again. I still had a few T3s left so I wasn’t too concerned. Well, the T3s ran out really fast. At one point when my pain was pushing 9.5 out of 10, I took T3s, up to 4 at a time and washed that down with a ml of CBD and another of THC. I also had some alcohol to really wash it down. I was then able to sleep, but I couldn’t keep that insanity up for long. So, back to the my regular medical clinic for some more T3s.
I also went back to the other clinic, the one that prescribed the CBD and THC for me. I had a consultation with an MD there and we basically agreed that CBD was not going to work for me. Clearly, it doesn’t work for everybody. I may still try using THC, but only at bedtime, and only if I’m feeling I need it for putting me to sleep. I may cease taking it altogether.
I’m quite sad about this because I had high expectations. At the moment all I can do to keep my pain levels down is to do very little of anything. Obviously I can write, but walking is even difficult and going out to socialize is increasingly unpleasant. Damn it, I love to socialize! I still go out and do volunteer work and maybe go to a restaurant now and again, but I have to rest frequently.
I knew that CBD and THC had not been tested using double-blind studies, but I hoped they would work anyway. Unfortunately for me, that wasn’t (and isn’t) the case. I sincerely hope they work for you.
It seems odd for me to describe myself as a cancer survivor. Oh, I had cancer, alright. In 2002, very early in the year, I was diagnosed serendipitously with kidney cell cancer. I had gone to see my GP about acid reflux so he sent me to to the hospital to have an ultrasound to check it out. The ultrasound tech wasn’t looking for anything in particular is my guess, but she zeroed in on my left kidney and sure enough there was a lesion there that they strongly suspected was kidney cell cancer. The techs didn’t tell me that, of course. They don’t discuss the results of a scan with patients in my experience. My GP was the one to break the news to me. His office called me to tell me the doctor wanted to see me at 5:30 the following day. I didn’t think much of it at the time, but in hindsight, that was an unusual thing for my GP to do. In any case, he broke it to me and said that the best chance of a full recovery for me was surgery as soon as possible. Then he sent me off to see the urologist who would perform the surgery. They didn’t perform a biopsy they said because of the fear of spreading the cancer which at that point was restricted to my left kidney. Fair enough.
So, after all the preliminary tests were done and I had seen the surgeon and the anesthesiologist my surgery was scheduled for the third week of February. Normally, of course, I would have been teaching at that time, but that wasn’t going to happen so the college arranged for subs on very short notice, one of whom was to die of cancer a few years later. The thing is that there are no obvious symptoms with kidney cell cancer. As far as I know, it doesn’t usually affect kidney function, so my kidneys didn’t show any signs of stress or disease. I felt fine. I did some work around the property. It so happened that we were just in the process of buying a new place in Cumberland, BC when I was diagnosed. There was a lot to do. We had an acre of property with the house and several outbuildings. It was a good thing that I wasn’t particularly debilitated. That was to come later.
Needless to say, a cancer diagnosis is traumatizing for everyone involved. I was concerned for my family as much, if not more, than for myself. Strangely, I was convinced that this cancer wouldn’t kill me so I was pretty upbeat about the whole thing. Why I felt this way I have no idea. It could be I was in denial. We humans are great at denial, even me.
Finally, I had my day in the operating room. I arrived at the hospital with Carolyn early in the morning with hardly anyone around. We said our goodbyes and I was taken to the pre-op area. They didn’t waste any time getting me ready and into the operating room. That I remember. My GP was in attendance and assisting, although I didn’t see him in the operating room at the time. Later, my GP told me that the surgeon had cut me in half laterally on my left thoracic area so that the kidney could be gently lifted out helping to keep the cancer contained. He said it was quite daunting. That’s what happened. Since then I’ve made do with one kidney. One of my former students was a nurse in the OR. We joked around until the anesthetic kicked in. Having a former student in OR isn’t unusual because many of my students were in the nursing program and were taking my sociology courses as electives. It happened again last year when Carolyn went in to have her appendix removed. My former students are everywhere!
I tell you all of this so you get a sense of what I mean when I say I’m a cancer survivor, but I find it hard to describe myself as such. I think of cancer survivors as people who have had to struggle for weeks, months or years on chemo and/or radiation, losing their hair and being in horrible pain the whole time. I have known many people who have succumbed to cancer, but I also know a number of people who have fought it, and fought it valiantly for long periods of time and survived. My cancer recovery was not at all long and drawn out. The surgery put an end to it. Done. Well, mostly done. My surgery was seventeen years ago and my left thoracic area has been a source of constant pain since then, aggravated often by the slightest movement. The pain in my side never lets me forget about the cancer that almost claimed my life. It gets pretty tiresome at times and saps my energy, but I carry on because what else is there to do? No, suicide is not an option.
So, I guess I’m a kind of cancer survivor, but I won’t be a life survivor. No one has ever been, nor will anyone ever be a life survivor. Nothing can ‘cure’ us of death. My surgery has allowed me to live longer and that’s fine, but I’m still in line for dying. And that’s fine. I don’t have any illusions about life and death. Life demands death. Life cannot happen without death. Denying that gets us nowhere. So, every day is one more day to enjoy and struggle over. When it’s done it will be done. That’s it. I know that some of you might think it odd that I say it, but if I had died on 2002, that would have been fine too. Carolyn and my family would have been sad and would have mourned my loss, but they would have gotten on with their lives. That’s what we do when people close to us die, we get on with our lives until our turn comes.
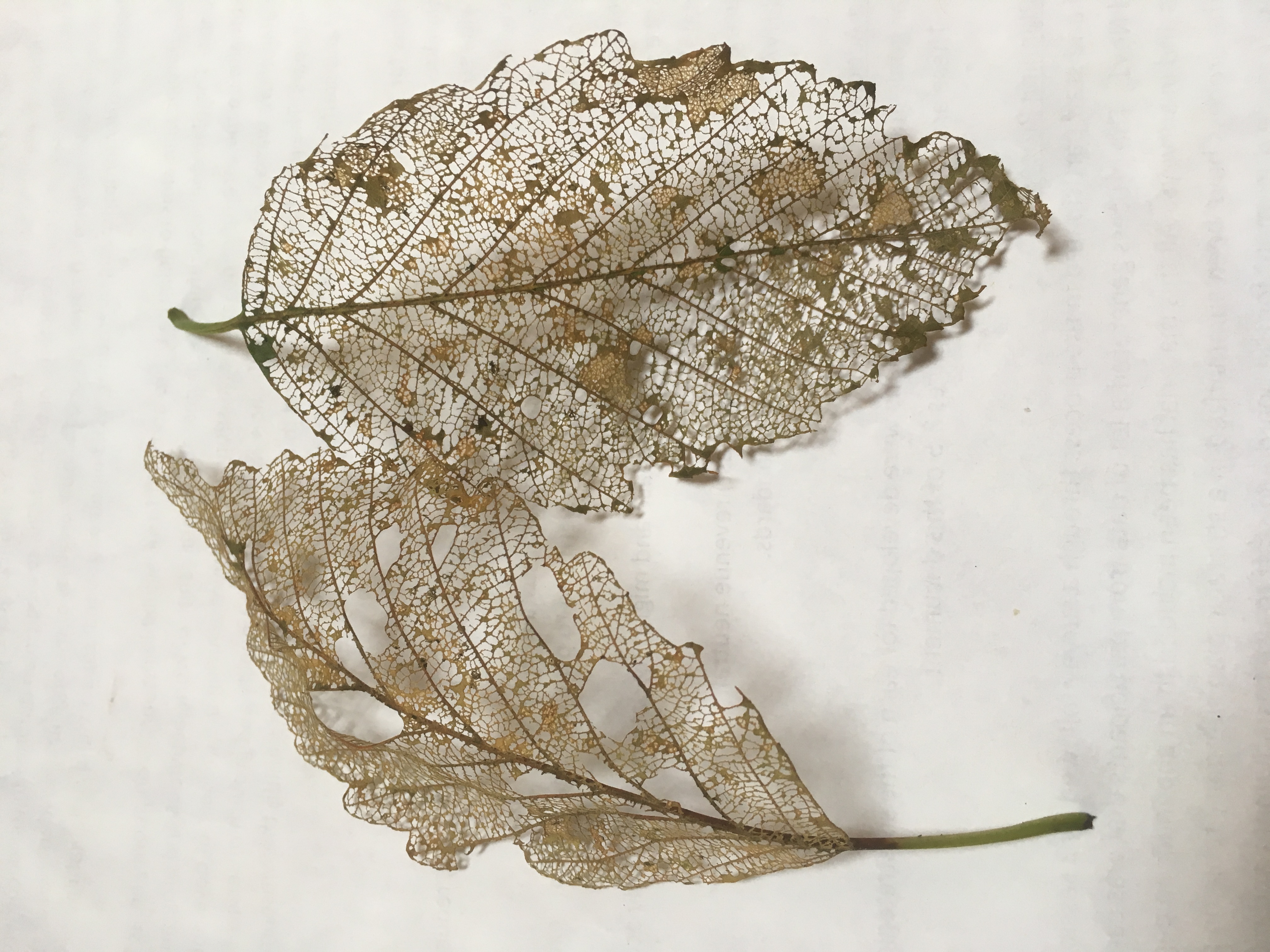
The photograph above is of skeletonized alder leaves caused by alder leaf beetle larvae. The adults chew holes in the leaves while the larvae leave the ‘skeleton’ of the leaf intact but strip it of the ‘meat’ of the leaf.
We have several alders on our property and they all look terrible with leaves dropping or dead but still on the tree. From what we’ve read on the internet the trees generally survive an alder flea beetle infestation, but I’ll believe it when I see it. Of course alders lose their leaves in the fall, but ordinarily, the leaves drop off in a heavy wind and are generally intact yet brown. The skeletonization of alder leaves is the product of the little black alder leaf beetle larvae. The effects of the two processes are entirely different and are obvious upon inspection.
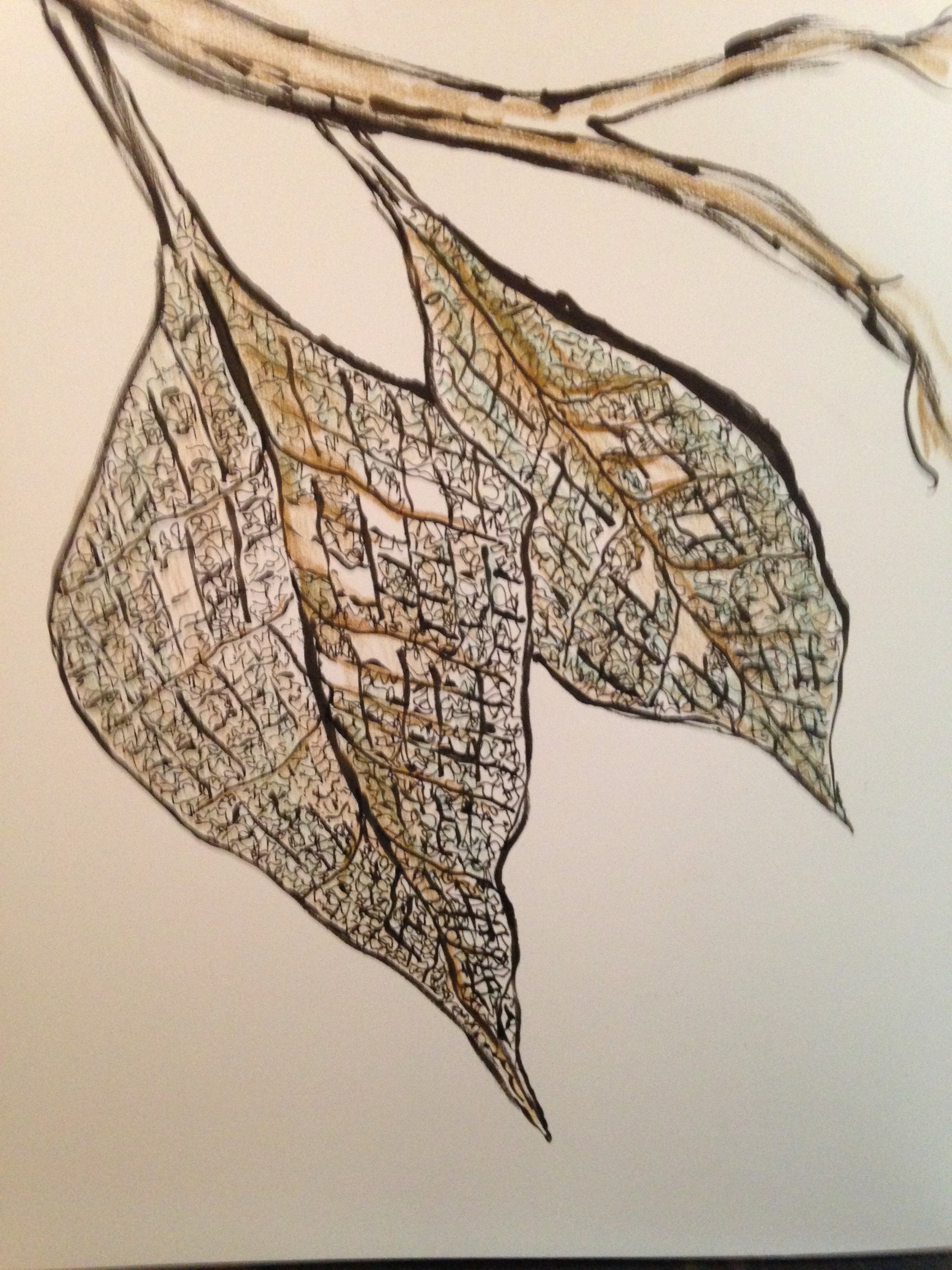
But enough technical stuff. The point of this post is that I find these skeletonized alder leaves quite beautiful. I love the intricacy of the connections of the veins. I love their strength. I haven’t used these particular leaves as a drawing subject, but I have drawn skeletonized leaves.
I can’t remember just when I drew these skeletonized leaves, which are not alders, but it was a few years ago certainly.
It’s difficult to see death in these leaves because we hardly see life in trees at the best of times. Forest companies don’t deal in trees, don’t you know, they deal in ‘fibre.’ When we see a load of logs on a logging truck going down the highway we don’t think of death (if we think of anything at all) related to the truck and its load. I have no real evidence to write this, but I do understand the culture and the language that denies death and this has that culture and language all over it.
That said, there is death in these leaves. They are dead or at least fully within the process of disintegrating and becoming compost for future plant growth. Their ‘meat’ is gone and all that remains is their ‘skeletons’. I find beauty in skeletons. I’m not sure why. We have lots of bones around here, bits and pieces from various deceased animals including a mouse, a tiny bird, raccoons and deer. Skeletons, for some reason, at least clean and bleached ones, have a simplicity and elegance that is always hidden in life. They require death to release them from their ‘meaty’ cover, to bring them to our attention, and to give them life. Maybe that’s why I find them so attractive.
Did you know? Children in lower income families (22.6%) are less likely to obtain a university degree than those in higher income families (59.3%). By responsibly using new data sources, we provide Canadians with greater insights.
Statistics Canada puts out a report every day called The Daily. Lately, it’s added a new feature to The Daily called Did you know? I quite like this new feature.
The observation about the relationship between education and family income comes to you courtesy of The Daily. It’s a simple statement of fact based on the masses of information on us that Stats Can collects. Of course the devil is in the details as they say. I’d need to dig a bit deeper into the Stats Can website to determine what ‘lower income’ means and also what ‘family’ means. It’s not as simple as it seems because Stats Can has different ways of determining family.
But let’s just leave it at the basic level it’s presented to us by Stats Can and think about why children in lower income families are less likely to obtain a university degree than children from higher income families. Let’s see how this basic fact can be explained by various political groups or parties for their own ends and what ‘greater insights’ Canadians might get from contemplating this fact.
If I subscribe to a Social Darwinian ethic with roots going back to Thomas Hobbes and John Locke, I might just argue that the greater numbers of upper income progeny going to university and getting degrees is the natural order of things. They are ”successful” because they are superior to the lower class rabble. They have the personal traits that make them successful, traits that the poorer schmucks down the road lack. Personal initiative is everything. Poor people just don’t have any of it. They are lazy and must be prodded to get them to work or to study.
If I count myself among the ranks of ‘progressives’, I may very well argue that the reason that poor people don’t go to university is that the social odds are stacked against them. They lack the financial resources to attend university. They don’t have the advantage of having attended superior elementary and secondary schools. They don’t have a home life conducive to reading or intellectual work, and their parents are probably people who don’t value a higher education.
Others along the ‘progressive’ spectrum put more emphasis on structural factors that impede access to higher education for low income people. For them, the class system steers individuals along certain pathways. It divides us and ensures we remain divided by selectively supporting certain social programs and not others. Social inequality from this perspective is not about individual differences. It’s about class and other group characteristics.
So, Stats Can can produce numbers like this but the insight it generates is not objective. The insight is filtered through a number of screens depending on the ideological framework deployed to make sense of it. There is virtually no gain to be had in trying to convince a dyed-in-the-wool Social Darwinist that Marx was correct in his analysis of class, and vice versa, of course.
[BTW, putting together another post about the meaning of things. Maybe by Sunday or Monday.]