Sunday morning. The huge snowfall we had over the past few days is slowly yielding to the onslaught of warmer temperatures and steady rain. It will still be a few days before we can extricate the car from its cocoon of snow and ice but that’s fine because we can always use the truck to get around. Having two vehicles is a bit of an indulgence, but the security of a backup is important to us right now.
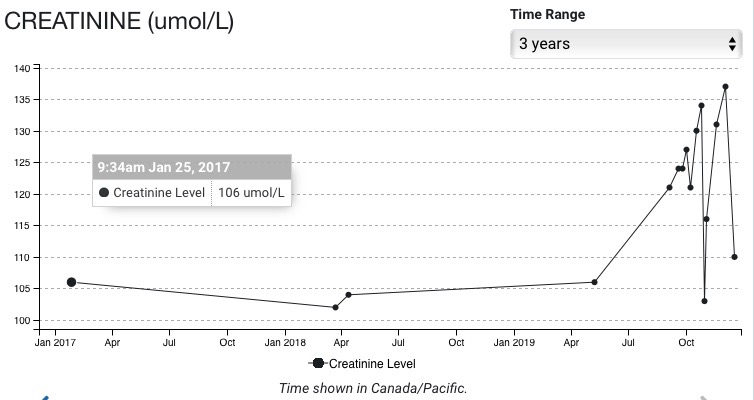
Every once in a while we hear a loud thump as large chunks of snow and ice break off of the load on the various metal roofs we have like a calving Alaskan glacier and crash to the deck or the ground below. Metal roofing creates a nice slick runway for ice and snow to slide off the roofs. We need to be vigilant when we walk under the eaves of the house or outbuildings for fear of getting walloped. I’m pretty safe though because I haven’t left the house in days, since my last visit to the hospital on Thursday actually. I’m having a rough time of it right now and I don’t rightly know if it’s because of the chemo or the myeloma. I know by my lab results on Monday that my hemoglobin counts are down and that means anemia is getting worse. Who knows why. I just know I’m exhausted for no goddamn good reason. I don’t mind being exhausted. Exhaustion can be a reward, actually, after a long run or a good workout. Being exhausted after sleeping all night and most of the day is not what I consider a reward.
I’m backing off my pain meds for a bit. I want to see where my baseline is. Getting the right dose of pain meds means constantly re-assessing pain levels. To be sure, pain varies a lot for me, not only in intensity but in kind. Lately I’ve experienced a dull, throbbing pain in my legs, particularly my right one. Every once in a while I get a spike of pain but that’s usually manageable. On my last visit to the hospital for my infusion of zeledronic acid, as I was sitting there in the chair with tubes sticking out of me, I got a cramp in my left side. I sometimes get cramps in my left side as an artifact of the surgery I had in 2002 to remove my left kidney. In any case, the nurses got very attentive all of a sudden as I writhed in my chair trying to find a comfortable position. They thought I was having a heart attack or something. It took me a while to assure them that it was just a cramp and not to worry. Pain is such a weird thing. I’ve had chronic pain for a couple of decades related to low levels of vitamin B12. Now, I have a hard time distinguishing between the chronic pain of the past few years and the new pain created by my myeloma. Not that it’s important, I guess, but doctors do want to know what kind of pain I’m having. I get pretty frustrated at times because I don’t know what’s causing my pain. It might be arthritis or degenerative disks too, but they don’t want to know about that pain. They want to know about pain associated with the myeloma. It’s not a simple thing to tell the difference. It’s funny: my orthopaedic surgeon in Campbell River asked me about pain in my right leg. I told him, yes, I have pain in my right leg, along my femur and even below the knee. Well, he said, that’s odd because your lytic lesion from your myeloma is at the distal end of your femur. Isn’t that where the pain is? Well, yes, but, but…
So, dealing with the symptoms of myeloma is one thing, explaining how I’m feeling is another thing entirely.
Some people love winter. They’re off skiing, snowshoeing, and doing other wintery stuff. I’m not a big fan. I’m a big fan of summer. You’ll never catch me complaining about how hot it is. Winter to me means short hours of daylight and long rainy nights. I am fortunate, though, in that we have a beautiful home to hunker down in and I have Carolyn as my caregiver. There’s always a hot cup of coffee ready for me in the morning and tea during the day. It’s clear I’m not the best of company a lot of the time but Carolyn is always there. I don’t know what people do if they don’t have community, family, and love, and find out later in life that they have incurable cancer. I’m feeling good knowing that I’m not on this road alone. Of course, dying is a lonely affair. You shouldn’t expect to have people accompany you into the grave like the Chinese emperor Qin Shi Huang Di, but having them along as companions until the last moments of life is as good as it gets in my books.