Who knows how much time I may have left to live. A week, a month, a year, two years, it’s all the same to me because after I’m dead, I won’t be around to regret or celebrate anything that happened to me while I was alive, including dying.
I had my last chemo treatment on September 15th. That’s it as far as chemo goes for me. On the 16th I had to go to the ER to reverse the damage to my body brought on by the chemo meds I took on the 15th. I wrote about my weekend from hell on my last blog post. I don’t need to go over it again. Now, I’m hoping that the damage caused by the chemo meds can be reversed sufficiently so that I can have a modicum of a life back. Frankly, I don’t hold out a lot of hope, but who knows? There are some hopeful signs.
Today is September 30th, 2022.
So, I’m only two weeks without chemo meds, but it seems that I already have more energy than I had while I was on chemo. I’ve had to bump up my dose of hydromorphone, but I’m not sure if that will have to continue into the future. The hydromorphone is essential for dealing with the pain I feel in my thoracic region. That pain originates partly from the surgery I had in 2002 to remove my left kidney, but the soft tissue mass that’s invading my back and left side may very well be contributing as well. I don’t know. All I know is that I experience a low level throbbing pain all the time emanating from there and every once in a while I get a pain spike that is intense to say the least. I’m no masochist, so I take pain meds.
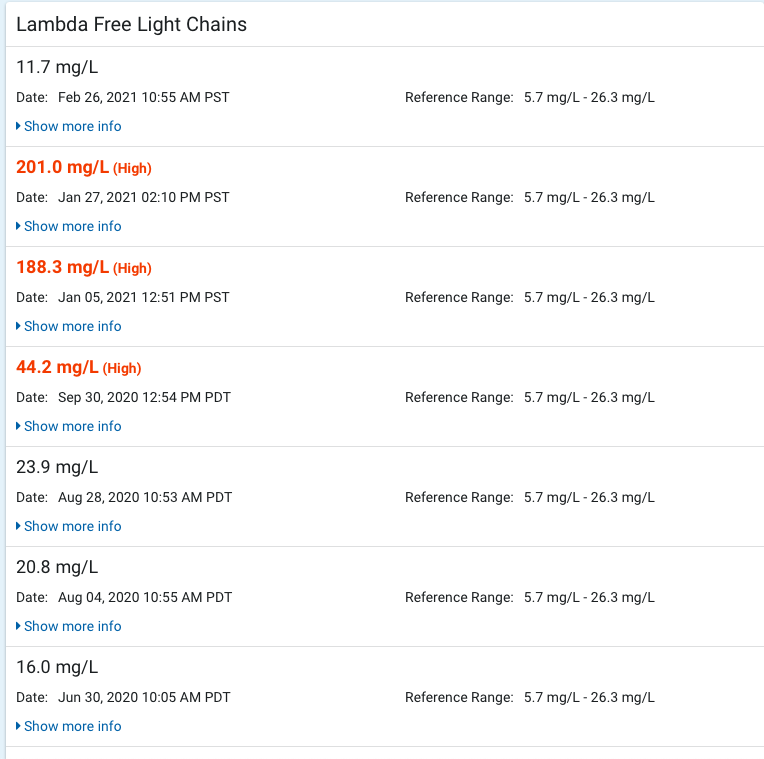
Because I’m not on chemo anymore, it’s unlikely the BC Cancer Agency will be concerned with my blood work. But, I’m concerned with it! It’s true that my symptoms should tell us how I’m doing and possibly give us some indication of how much time I have left to live, but blood tests are much more definitive and might give us a heads-up on how my kidney is doing, and how much crap I have in my blood. My GP doesn’t seem too keen on blood work either. Oh well, we’ll see about that.
I guess my biggest concern now is the uncertainty around how long I might live. In a sense it’s not a big concern because I should know when I’m on my last legs, but I may not. At the end I may decline quickly, especially if my kidney packs it in, but I may find that my last few days stretch into weeks or months. Whatever happens, because of the uncertainty, it doesn’t make a lot of sense for me to plan ahead, except in a general sense, for MAID for example. So, I live one day at a time. I get up in the morning and expect that I’ll still be alive in the evening when it’s time to go to bed. I watch news programs on YouTube, but I’m not invested in them at all. It seems as though the world is coming apart at the seams, but all the seeming chaos is moot as I face my own dying.
I can’t believe it’s the end of September. We’re moving into the Fall. The big maple in the front of the house is just starting to turn. The leaves change from green to a pale pink on the underside and bright red on the top. They fall almost in unison and cover the ground with a carpet of pink and red. There is dying in this process, but not death, not yet. The tree is preparing for its winter sleep, and will grow a fresh crop of bright green leaves come March and April. Death is in its future but it’s not for now.
The sword ferns are a different story. They have spores that are spring mounted on the undersides of the ‘leaves’ and that are flung out in a desperate search for a bit of fertile ground to sprout and grow. Chances are that none of the millions of spores will find a propitious bit of ground to grow into a new fern. Not to worry though because the fern itself will sprout new growth come Spring and just carry on. The ‘old’ leaves will turn brown and be displaced by the new leaves. They will create nutrients for the plant as it carries on. There is dying here, but not death, not yet. Death will come much later when the plant itself has no means of recreating itself, when it is exhausted and when the ground that is its home is no longer capable of sustaining it.
We have what’s left of a cascara tree in our yard, about six metres from the south corner of the house. It was a beautiful tree with a sculptural quality and a large canopy when we moved here in 2002. The tree itself was probably ten metres tall. We figured it had been growing on the property for forty years. Then one day it just up and died. The leaves all fell and the bark peeled off in strips. Its skeleton still stands. We hang Christmas decorations on it now. It lost its leaves every year like all the other deciduous trees on the property only to come back strong and vibrant every Spring, until that sad day a few years ago when it died.
Plants aren’t afraid of death and dying. They don’t feel fear. Yes, some people have anthropomorphized plants and have attributed to them human like feelings and motivations. That’s just plain silly in my mind.
Truth is, no matter who or what we are, we die. Simple. But like most animals we fear dying. Trees and plants in general have a different relationship with dying and death than animals do. They cannot flee from threats to their lives. They die every Fall only to be revived in the Spring, but even they ultimately meet their end when they reach the limits to growth. It could be argued that we follow the same trajectory except that we can successfully flee from threats to our lives, at least to some extent.
To me, cancer in old age is natural, and part of the deterioration that many organisms experience in the final stages of life. I love my life, but it must end. My body has decided that its exit from life will be via cancer. How can I argue with that? I tried to argue with it by using chemotherapy, but unsuccessfully. Now, it will countenance no significant opposition. Such is life.
___________________________________________________________________