In my last post I mentioned that I’ve put together one hundred and fifty thousand words on my blog since I was diagnosed with multiple myeloma in the fall of 2019.
Looking back on my many posts, I’m now concluding that I’ve said pretty much all I want to say about my relationship with myeloma. There may be a few more details I can profitably address such as increasing levels of pain, and Its location, but I have myeloma, there’s no question about that, and it’s going to kill me. Now that I’m palliative and not under the care of any oncologists, I feel that all I have left to do is take a schwack of pain meds and wait to die.
Thursday, Jan. 12, 2023 – ~ 11 AM
This morning I got up at 7 or so in anticipation of going to the hospital for a lab visit. I was feeling just fine until I went into the bathroom to ablute. I got my gear out, but while I was doing that, I felt a twinge of pain in my ‘gut’ area (generally in my midsection, right through my body.) Soon, that twinge developed into generalized pain severe enough to take my breath away). Then it ramped up to a 9 or so on the 10-point scale. As soon as I realized that the pain had got to a 5 or 6, I started taking hydromorphone breakthrough meds. I took three times as much as I would normally take. I also took some dexamethasone (8 mgs). I was supposed to take 4 mgs). I also took some acetaminophen (1000 mgs).
It took an hour to an hour and a half to settle the pain down to a 4-5 on the 5-point scale although at the time I thought that the pain would never attenuate. I thought that dying at that point might be a good idea.
Pain, in and of itself is not a bad thing. It signals that something is wrong in the body that needs correcting. (This is a perspective inherent in the pathological end of the medical spectrum.) Pain may never be eliminated from a body.
Earlier I wrote that: ‘Now that I’m palliative and not under the care of any oncologists, I feel that all I have left to do is take a schwack of pain meds and wait to die.’ Well, what of that?
We all wait to die. But we’re not supposed to do that, don’t you know? It just isn’t right. We’re not supposed to just sit around waiting to die. Actually, it’s downright immoral to just wait around for anything, especially for dying. As humans we’re meant to move around, to get ‘er done! Ironically, we go on vacation every once in a while with a major goal of sitting or lying around doing nothing. There’s a contradiction there, but we can ignore it if we turn away and don’t pay any attention to it.
People do get freaked out when they see people in care homes not doing a lot of anything. “Look at all the crumblies, laying around, just waiting to die! They aren’t productive. They can’t even clean their own bums.” We’re supposed to DO something, anything. “The devil makes work for idle hands” don’t you know?
Yes, true on all counts. But before we get all self-righteous, we should consider what is so morally superior about doing things. I’ve already written somewhere that, following Ernest Becker, we think of wealth and health as the two most important moral imperatives in our lives and in our civilization (although we very seldom think in those kinds of abstract categories).
Since we’re already primed for thinking about things on a ten-point scale, can we think about morality and health on a scale? Maybe using a scale where a 5 is average (the mean in statistical language) and the extremes are at 1 and 10? What would morality and health look like on a scale of 1 to 10? Caution: this analysis is simplistic in the extreme but it works on a very basic, silly way.
The scale would look something like this I think: If you’re a 10 you’re buzzing with activity. You can’t stop. You run marathons every week. You have two jobs, or you make money by investing in stocks and bonds. The downside about being a 10 is that you’re possibly on your third marriage because nobody can stand to live with you for any length of time. Thus, if you’re not actively pursuing wealth and are not super healthy, buff and running marathons, you probably suck. At 1 you suck a lot, at 3, yeah, you suck, but not irretrievably. If you’re a 5 you’re probably normal in our world. You probably have a decent job, and you do some exercise. Nobody’s going to look up to you, but, conversely, nobody is going to look down on you either.
If you’re a 1, you’re a slob, a poor slob. (Wink, wink, nudge, nudge).
Let’s look at this ‘distribution’ statistically.* If you draw a random sample of the population on a characteristic like height. you should come up with about 68.2% of the population who ‘fit’ within one standard deviation from the mean, or the average. Leaving aside height for a moment, in moral terms, if you’re on the left side of this histogram, you tend to the sucky side of life. On the other side of the mean you tend to the above normal side of life. You’re nothing special, but you’re a nice, positive person. You know, nice and positive. Further up the scale and we can detect sugar dripping from your lips.
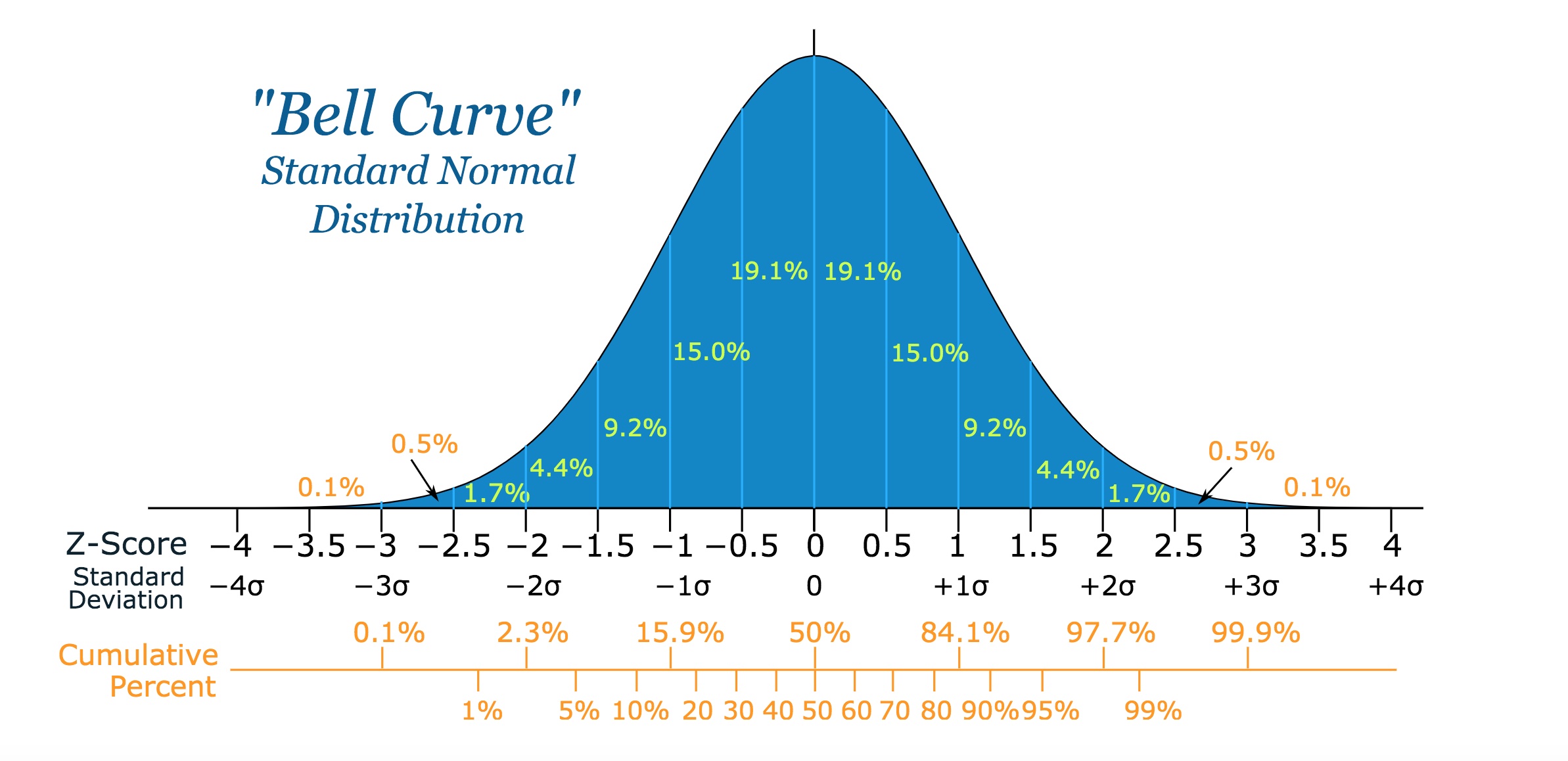
From: http://openbooks.library.umass.edu/p132-lab-manual/ Physics 132 Lab Manual by Brokk Toggerson and Aidan Philbin.
The further you get on the left side of the distribution, the suckier you get until you dissolve into a slimy pile of suck. It’s good that not very many people fit into that category because wading through slimy piles of suck could be downright tiring at times. The fewer of those around the better. Rain puddles are way better, in my opinion.
Well, this is all well and good. We judge people all the time, even the way we die. We live in a very strange world if you haven’t noticed yet. We are a very strange species.
If you want to stay on the good side of your civilization, keep busy and try not to let your knuckles drag while you walk down the street.
__________________________________________________
*I wouldn’t take ‘statistically’ very seriously here. Just having a bit of fun. Oh, the histogram is fine, but fitting morality and health into it may not be so fitting.
__________________________________________________
January 13, 2023.
Today is the fifth anniversary of my mother’s death. She died in 2018 at the age of 94. I miss her even though I barely saw her at all in the last few years of her life.