I taught university level courses in sociology and criminal justice for over 30 years but now I'm retired and at 72 was diagnosed with multiple myeloma, bone marrow cancer. This site is now a chronicle of my journey with myeloma.
What do I want to do with this blog? The thought crossed my mind that just giving up on it would not be the worst-case scenario. I’ve been at it for a few years now so it wouldn’t be outrageous for me to either quit entirely or maybe just take a break over the summer. Mygawd, I’m not making any money writing it. Lots of bloggers make money on YouTube with their blogs. I don’t, so what’s the point? Maybe I could monetize my blog, attach it to a video log and turn it loose on YouTube. After all, we DO live in a capitalist society. Might work. Probably not.
The weather has been wonderful lately if you want to lay about on a deck. I sit on the deck close to the rock/fountain and watch the birds come down for a drink. The one in the video here is a female goldfinch we think. She flits around avoiding direct contact with the fountain. It would probably knock her over if she did.
The wisteria gives them some shelter and protection before they come down to the fountain, but they’re still wary. Smart birds. There are cats prowlin’ around here. Our princess is one of them and she’s a hunter sometimes, mostly mice, but we don’t want to tempt her with birds. She’s being such a brat lately. She seems to have figured out exactly when I’m just about to fall asleep, then she pounces on the bed, meowling like crazy and poking my face with her paw.
Tilly has been hanging around the pond a lot lately. She patrols the perimeter sniffing around trying to get frogs to abandon their rocks along the shore. I don’t like the way she’s been fixated on frogs lately. She come close but she hasn’t caught any yet. I’d be very pissed off if she did. She spends most of her time under the deck these days where it’s cool. She’s got such a thick black coat she must really suffer in this heat, but she never complains.
Got a call from my Oncology GP this morning. He noted that my bloodwork is coming back from the lab within reference ranges (normal). Tomorrow I go to the hospital for another infusion of Daratumumab. After that, I don’t get another one until the end of August. As of this month, I’m down to once a month for the Dara. I keep taking my regular chemo meds, lenalidomide and dexamethasone, three weeks on, one week off. So, I’m in a weird space where I have no myeloma detectable in my blood, but I’ll be on chemo for the foreseeable future, that is, until the drugs don’t work anymore. At that point they’ll put me on another regime. That means that I must be vigilant around the side-effects of the chemo. It’s not always easy to tell chemo med side-effects from pain med side-effects.
For an old man, I’m feeling pretty good these days for about fifty percent of the time. I’m sleeping moderately well most of the time, but I have wakeful nights periodically. My neck is what’s tormenting me the most these days. According to my Oncology GP I have OAD (Old Age Disease). I can’t turn my neck more than 3% left or right. Maybe 4%. Makes it hard to do shoulder checks when I’m driving. Of course, I still drive. What are you thinking? I just have to turn my whole body when I do a shoulder check. That’s fine.
Technically, I have degenerative disc syndrome and it’s common among older people. I’m getting a CT scan early next month to confirm the diagnosis. Once I get the scan, I can ask my GP for a referral to someone who might be able to do something for me. That would be good. If I do get some relief, I’ll be able to do more writing, and maybe some sculpting. I’d love to do a bit of printmaking too. Or maybe I could just lie on the couch more comfortably. That would be good.
Wayne Bradley passed away on April 3rd of this year. He was informed by his GP in mid-March, after a consultation and imaging that he had a growth on his pancreas and nodules on his liver. Pancreatic cancer metastasized to the liver is absolutely unforgiving especially with a late diagnosis. It has the reputation of being a cancer that kills quickly. In Wayne’s case there was barely three weeks between diagnosis and his death at the hospice in Comox.
Wayne was two years and a day younger than me. We were both involved in social activism of one sort or another. You may have seen Wayne with Janet (his wife) selling coffee and chocolates at various events in the Valley. Carolyn and I were quiz masters at the Cumberland Forest Society’s trivia nights some time ago now, on one occasion, Wayne and Janet were there at the back of the hall with a table set up to sell World Community products. They only did the coffee and choc sales once at Trivia but had those sales regularly at Miners’ Memorial events such as Songs of the Workers.
The last time I spoke with Wayne was on our deck on the occasion of a Home and Garden Show in 2019. This was Carolyn’s last appearance in the Cumberland Forest Society Home and Garden Show. We sat around drinking tea and chatting. I was not doing well at that time and a diagnosis of multiple myeloma in October provided the reason for my ill health. I recall that Wayne was very keen to talk about electric vehicles. We were definitely interested in electric vehicles but were cautious about making that kind of investment one of the reasons being that the property was not wired for it. It is now, but we’ve moved on because of my cancer diagnosis and other reasons.
My type of bone marrow cancer leaves me completely exhausted and dizzy. That, on top of the pandemic, made it so that we were pretty much in isolation. So the summer of 2019 was the last time we saw Wayne and Janet. We (our son-in-law) bought tickets to the World Community Film Festival this past February but that was an online event.
Wayne suffered from abdominal, back pain and utter exhaustion in the last weeks of his life. That is common with pancreatic cancer, but Janet told me that strokes are also common with this disease. I had no idea. Wayne suffered a debilitating stroke on March 30th, and he was gone in just a few days.
Death in these circumstances is expected but still shocks. We all die, but the circumstances will have something to do with how well the family is prepared for a close relative dying. My type of cancer is treatable with chemotherapy and can go on for years, plenty of time to prepare for dying but when I die I’m sure it will still be a shocker for the family. Unlike myeloma, pancreatic cancer doesn’t generally allow for years of grieving. In a way that may be a blessing.
Wayne was a great guy. He was committed to his community and worked tirelessly for the good of his community but also for communities far and wide, those involved in the coffee and chocolate trade. Janet was Wayne’s partner at World Community but both were involved in other initiatives over the years. They were seldom far from the action.
Hearing of Wayne’s illness and death was certainly a shock. Cancer is often very difficult to diagnose and once diagnosed it’s often too late to do anything about it. According to Johns Hopkins Hospital, eighty percent of pancreatic cancer patients are diagnosed at Stage IV, when the prognosis is bleak.
Wayne will be sorely missed by family, friends, colleagues, and acquaintances. He was a man of integrity, strength and determination. He was a good man.
I was thinking of writing a timely, thoughtful blog post for my last one of the year, then the pain around my jaw went a long way to discouraging that. Yes, I feel that there is something quite wrong with my jaw, a wrongness likely associated with myeloma.
I went to see my dentist a while before Christmas because I thought the pain in my jaw and the increasing numbness there was tooth related, but it turned out on closer inspection by a specialist that the lesion there is probably myeloma related. Such a ducky way of ending 2020.
Interesting! This is my seventy-fourth post on my experience with myeloma and it turns out that Monday is my seventy-fourth birthday. Coincidence? Of course. There’s no way I could engineer my life that closely.
I suppose I’m happy that I made it to my seventy-fourth birthday although with everything that’s going on these days, it’s hard for me to get too celebratory around my birthday.
Frankly, I’m much more concerned with what happens on January 5th, the day after my birthday. That’s when I get my blood tested for the presence of myeloma protein and other noxious nasties whose only goal in life is to kill me. I was found to be in remission when my blood was last tested three months ago. Now, we go at it again. We wait and see what the verdict is. I must say that this is getting somewhat irksome.
Oh well. So far this post has been about me and my problems. No sociology and no profundity. Just a little whining and sadness. I think I’ve earned it. But it does stop here.
BTW…I hope for your sakes that 2021 is at least twice as good as 2020.
Yes, today is World Kindness Day, a holiday celebrated in many countries since 1998. It’s also Friday the 13th, but let’s ignore that for the moment. You’ll be pleased to know that there’s a World Kindness Movement too. It’s front and centre in the kindness celebrations that are held in many places around the globe today.
I promised one of my blog readers that I would write about kindness sometime. This is an opportune time to do so. She also wanted me to write about recognizing others, a gesture that gives their feelings a boost and their existence added social value. To be snubbed is to be humiliated, as is being chosen the last player for the pick-up soccer team on the neighbourhood pitch after school. We yearn to be recognized and not ignored. There is an element of kindness to acknowledging others in social situations or at any time for that matter.
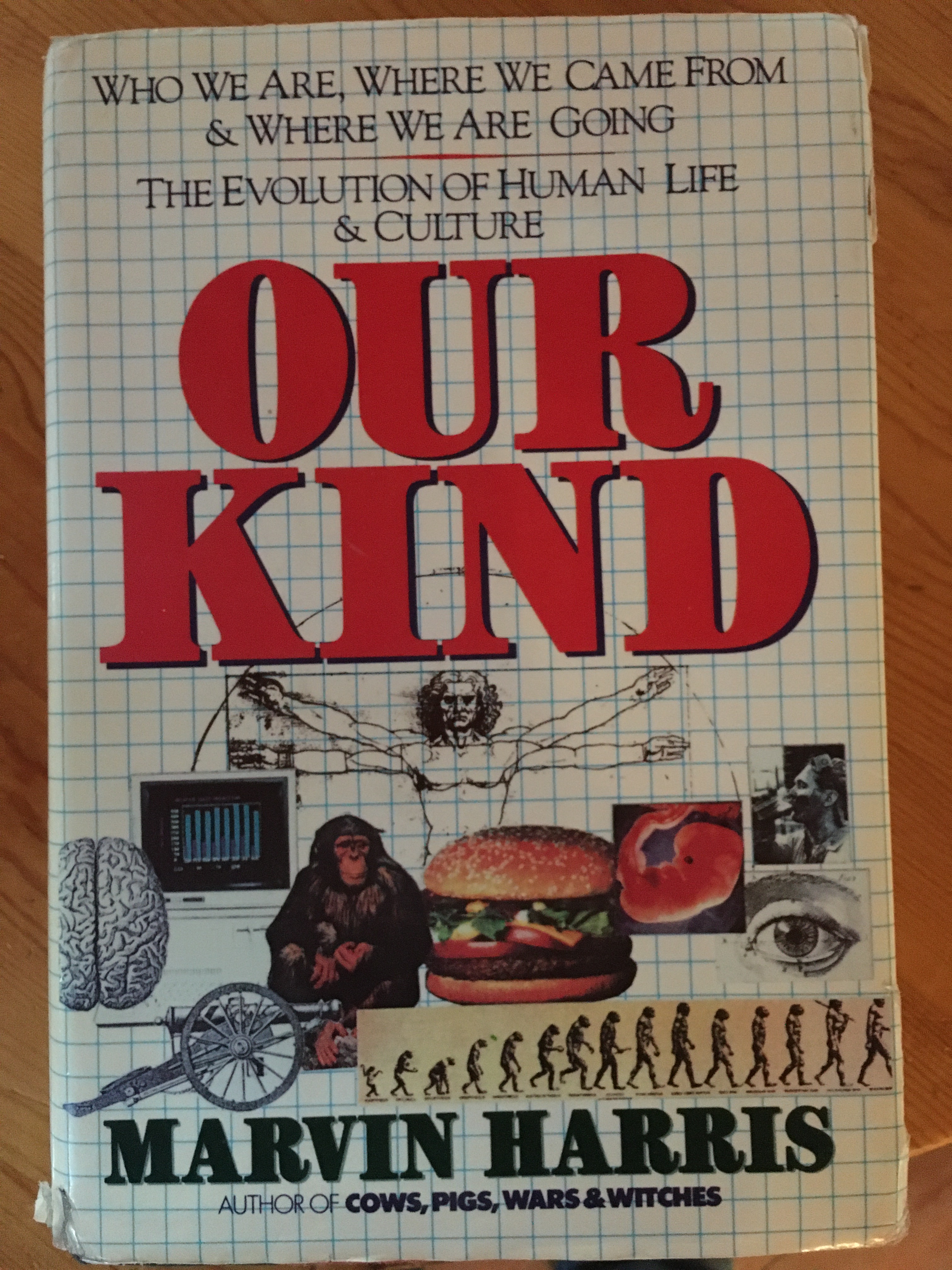
But what is kindness? Miriam-Webster defines kindness thusly: “the quality or state of being kind”. Well, that helps a lot. So what is the definition of kind? Miriam-Webster replies: “a group united by common traits or interests.” But wait, this is the definition of kind as a noun as in ‘what kind of car do you drive?’ So, what is the definition of kind as an adjective? Miriam-Webster helps us out again: to be kind is to be of a sympathetic or helpful nature.
Well, okay then: to be kind is to be sympathetic or helpful. That’s generally how I would use the word. However we still have to reckon with the noun variation of the word. The image below is of Marvin Harris’ Our Kind, a book he published in 1989 as a project designed to help educate college students (among others) who, at the time, were unable to recognize the boundaries of the United States or know who’s side the Soviet Union was on during World War II. Our Kind is a compendium of what makes us human, of “the evolution of human life and culture” according to the cover.
Humans are of one kind in essential terms, we are one species after all, but we are still divided in a myriad of ways. We are one with our kin (a word akin to kind) but the further away we get from our kin (our sibs), the less we feel bound to be kind to people. Who are the people we can expect kindness from? People who are kin to begin with, then anyone we can define as part of a kin-like group, a group that can be defined socially, politically, geographically, or in whatever way we decide qualifies as a membership pass.
The reader who suggested this topic to me is genuinely concerned with the divisiveness and viciousness of much of what passes for social and political discourse these days. The lack of civility is glaring in some quarters to the point where conversation is impossible. Shouting replaces discourse.
Harris, in the 1980s, was dismayed at the low level of civility and kindness exhibited by a large percentage of the population. He doesn’t say it, but I will. There will be no possibility of kindness, sympathy, and civility enduring as basic human values until we break down our current social and political boundaries and accept each and every human being on this planet as one of ‘our kind.’
It’s as simple as that, but as complicated as that too. The reasons we divide ourselves so earnestly into political and social groups according to Ernest Becker is partly as the basis for competition, competition designed to separate the winners from the losers in the eyes of the gods.
At the moment we are witnessing massive cleavages in the fabric of American society, cleavages that seem to be politically defined around political parties, but which are essentially about who qualifies for assent into the realm of the few divinely chosen. The religious has infiltrated the political in American society to the point where ‘opponents’ are seen as evil incarnate and where anything less than total victory is unacceptable and will not be tolerated because the alternative is death.
I am not particularly optimistic about American politics or about global politics for that matter. I don’t know if there is the will necessary to unite people and to set aside divisions of politics, class, race and sex so as to see everyone qualify to be included in our kind.
There seems to be plenty of will for division with the vast majority of social institutions organized to divide. Are things as dire as I portray them here? No, they aren’t. After all there are strong unifying forces in the world too.
Maybe more on this later. I’ve written about this before if you care to peruse my archives you’ll see what I mean, but I’m also willing to explore more fully some of the themes introduced here, particularly those around competition and division. These have an ‘animal’ dimension as well as socio-religious ones.
Carolyn has her hands full these days, does she ever. I’m experiencing some particularly nasty side effects of one of my chemo meds weakening my legs to the point of near collapse, and last week we found Princess, our cat, in severe distress requiring long stays at the vets and heroic efforts to save her life. On top of that, there’s the puppy we brought into our lives. She’s a wonderful addition to the family, but she’s a rambunctious puppy, demanding of attention and needing some training to stop her from biting us incessantly, ripping our clothes and our bodies. Then there’s the garden.
The Garden
Speaking of the garden. It’s unbelievable this year. We’ve been eating lettuce from the garden for weeks but now the peas are coming on strong and the broccoli, cauliflower, and kohlrabi are in the pot. Some of the raspberries are ready to pick, the tomatoes are coming on as well as the zucchini and cucumbers. We’ve never had much luck with root vegetables, but this year it looks like the potatoes, carrots and beets will produce lots of tasty treats. The garlic is a bit behind this year but should be ready to pick in a week or so.
The cedar trees are loaded with cones this year to the point where they’re dragging the branches down. My favourite flowers, the lilies, are opening everywhere on the garden and this year we have a rare pond iris bloom. Such a delightful show! The birds are active too and the squirrels are busy picking the not-yet-ripe cherries. Looking out the living room window right now I’m seeing an American goldfinch, a purple finch, a couple of woodpeckers going after the suet attached to the feeder and a congeries of species, mostly thrushes, towhees, chickadees, and finches. At the pond is where we more often see kinglets and warblers. Of course, hummingbirds dash about in their usual frenzy all over the garden. So much to eat these days for all the birds.
Cedar cones, lilies busting out, miniature mock orange, pond iris, and brassicas.
Me
It’s been tough lately. I’m in quite a bit of neuropathic pain from one of my chemo drugs, something I’ve already written about a couple of posts back. My legs want to give out on me and if I should ever get down on the ground, I can’t get back up on my own. It’s downright discouraging. One of the main problems with this is finding the right pain med to deal with it. Hydromorphone is ineffective against neuropathic pain although I’m always tempted to take it so that I get stoned enough to be able to sleep. But I don’t like that strategy so I’m looking to other ways of getting by. I’m cutting back on my hydromorphone and taking more acetaminophen. That seems to allow me to sleep better while avoiding some of the worse brain fog and intense fatigue that I get from the opiates.
It may be that some of the back and leg pain I’m feeling is from conditions other than those produced by myeloma or chemo. To see if there’s a mechanical issue, my local oncology GP has ordered an MRI to check things out. He also suggested I think about taking Gabapentin or Lyrica, but I’m not having anything to do with those drugs. They may help in some ways, but they can create lots of problems I don’t need. I’m talking to the palliative care people too and they may have suggestions. In the meantime we wait and hope the pain attenuates. I’m operating at a very reduced capacity at the moment. Must carry on, though. No point in quitting now.
Thank goodness I have Carolyn and the garden for solace.
Princess Pretty Paws
Princess is at least ten years old and has been very healthy since we got her two or three years ago. Last week we got the puppy and Princess disappeared. At first I thought there might be a connection, but Princess is not the kind of cat to run away. In any case, Carolyn found her upstairs a few days ago. She was obviously in distress. We think that she may have been hiding out in the crawlspace as she got sicker and sicker. So Carolyn immediately took her to the vet. Princess stayed there a few hours for observation and tests. The vet was at a loss to figure out what was wrong with her. The one real anomaly in her blood was a high bilirubin count indicating a liver problem. We thought it might be poisoning, but that wasn’t the case.
It turns out she has a serious problem with a bowel infection or something along those lines and she has inflamed organs. So what to do? Well, some people might have decided to put her down but that’s not our style. More tests and more again. She saw the vet three days last week as well as today, on Sunday. We have a great vet!
Princess has been on a feeding tube for three days now and we seem to have that under control. She’s on lots of meds that we give her at feeding time. Her fever has dropped, she’s eating (through the tube) and she’s getting more active. She’s not throwing up and she’s using the litter box. All good signs. So we carry on and see how it goes. We keep our fingers crossed. No point in giving up on her now!
Matilda (Tilly)
Matilda (Tilly)
Tilly is a Bernese Mountain Dog, Shepherd and Maremma Italian sheep dog cross. She’s nine weeks old and is a gift from our amazing daughters and their families. She has a great personality but like most puppies of that age is teething and biting is something she does indiscriminately. She plays rough. She bites whatever comes along: cardboard boxes, chewy toys, table legs, blankets, and us, of course. Carolyn’s arms are scratched up quite badly as you might expect. Mine are less so. We’ve found some puppy social classes for her and with some training she’ll be just fine. She’ll grow into a wonderful, mellow girl. For the moment though, she is a handful. There’s no turning our backs on her for a second. She’s very fond of the fountain next to the deck and lays on the rock taking a nip at the fountain from time to time. She’s figured out how to get under the deck and she goes from one end of it to the other under there. She figures that’s a real hoot. She loves her treats and is now responding readily to the sit command but she might just ignore that if she she wants to play, meaning attack and bite us. To be fair, she can be gentle too and plays by herself quite well. She’s not always bitey.
We’ll have to be very vigilant when Princess starts wandering around the house and property. We don’t want Tilly chasing her. It will be a challenge.
So there’s sorrow in the household at the moment but there’s a lot of joy and hope too. Be careful out there in the Time of Covid-19!
Think you can identify them all? Some are duplicated and there are frames with more than one type of flower or plant in them. I can’t identify most of them. It’s Carolyn’s garden!
Before I do that, however, I want you all to feel free to contact me. If you have problems with privacy i.e., you don’t want your comments to appear in public, please let me know when you post comments, or pm me on Messenger or you can email me at rogalb@shaw.ca.
Things can change very quickly these days and positive things do happen! Oh, I still have myeloma and I started chemo yesterday. That seems fine. The pain in my neck has attenuated too. Who knows why. I can feel it lurking around my cervical spine, but for now it’s keeping a respectful distance. I can actually type and stay relatively focussed. I pay for that by not taking as much hydromorphone. AND my kidney is back to normal…for an old guy like me anyway and that’s very good news. I was thinking I may need a wheelchair to get around and we were making arrangements for that, but for the moment, I’m good. I’m feeling okay at the moment, ten times better than I felt two days ago, but that’s how it goes with chronic pain. Things can easily go back to shitty in a flash. Of course I know that I’m an old guy with cancer and I can see the exit door over there just beyond the bright white light, but I can’t see the handle yet, so I think I have some time. Besides, I can put that to the back of my mind. It doesn’t help at all to focus on things I can’t inevitably change and stick to the things that can get me, and others, better quality of life now and for the near future.
So, pain. My last blog post was about Carolyn’s experiences at the Emergency Department here in Courtenay. My penultimate posts were about my visit to the oncologist in Victoria and my subsequent disastrous ER visit the following day. I sit here somewhat unable to piece together accurately in sequence what happened to me since last Wednesday. Truth is I’ve seen two specialists since then, have had a ct scan with another one scheduled for tomorrow which showed that I have severe disk degeneration in my neck that is, along with arthritis, creating the pain vortex in my neck. My neck pain has been a roller coaster of severity. I have a neck brace that helps with that too as you can see from the photo below. Hi!
My office
Now, this is where it gets interesting because my oncologist tells me that my neck pain has nothing to do with my myeloma. It has everything to do with my disk degeneration and arthritis. So, I ask: does the myeloma contribute at all to pain in my body? Of course it does, comes the answer. It attacks your bones. The ct scan did not find the right kinds of lesions on my cervical spine, so they were not the source of my neck pain. Well, okay. I guess I can go along with the argument that my nasty bulging disks are responsible. I mean I had surgery on my lower back decades ago to alleviate a ruptured disk problem so I’m familiar with that. Still, recently I’ve had over the top thoracic skeletal pain which really was caused by my myeloma so whatever. I’m getting a ct scan tomorrow to check that out among other things.
So, what I’ve been able to piece together through moments of excruciating pain and hallucinating sedation, is that the pain I’m experiencing the most severely seems to be concentrated in the bony/connective parts of my body that had already suffered trauma. I’m thinking specifically of the area on my left thorax where my kidney as removed, the lower back cervical area where I had a disk removed, the left heel where I had planers fasciitis, that sort of thing. My neck too and my shoulders where I had rotator cuff tears, both sides due to falls and long term overuse issues.
I started asking this question to whoever would listen: is there an association between myeloma and increased intensity of pain in areas of previous bone trauma? Answer: I don’t think so, but probably not. Question: Do you know of any research between myeloma and where it affects the body most? Answer: Not that I know of. I had a chat with my daughters about this. They’re no slouches when it comes to research: One of them works in the field of non-profit housing and the other in biomedical research. They are my truly trusted experts. But, I have access to a lot of material too because I’m still associated with North Island College as emeritus and have library privileges.
Okay, that still leaves me dealing with my own experience of pain and those of others (read the comment by Tanya Wood based on my last post), some of whom have chosen to remain anonymous. I’m especially concerned with Emergency Departments and with receptionists (gatekeepers) in GP offices who, I know are just doing their jobs, but who, when I call to simply ask that can the doctor just tell me if I can increase my dosage of hydromorphone says: “Well, the doctor will have to see you for that” To which I answer: I can barely move. I have excruciating pain and can barely get out of my chair. Can he just tell me quickly about increasing my already existing prescription with pills I already have?” “Well, no, the doctor will have to see you.” So, I couldn’t take anymore of that and told her we’d get back to them. Later, Carolyn called and talked to someone else who said someone would be in touch. My doctor called me later in the day when he had done his patient visits for the day, something he as often done in the past and I knew he would do again. So, all day I was left figuring out how many more hydromorphone pills to take before overdosing. I’m not at all suicidal, so that’s a concern. I’ve known of many people who have died from accidental overdoses. I wasn’t about to be one of them, but my pain was so intense it was a good thing I wasn’t standing at a subway station waiting for a train anytime last week. I may just have acted compulsively and jumped onto the tracks. Of course that’s a little hyperbole, but that’s okay among friends, isn’t it?
I wrote to Tanya Wood (who’s husband, Darren, died a couple of years from complications resulting from a tragic accident) in response to her heart wrenching comment that ER departments are microcosms of our culture. They operate using the same moral assumptions as everyone else in society. We have deep-seating cultural aversions to death and disease. Most of those are built on our huge biological insecurities. I paraphrase here Ernest Becker who wrote something like: Disease takes away our ability to enjoy the pleasures of life and death does that permanently. He calls death and disease the twin pillars of evil for us. [You need to read some of my early posts to get a sense of how brilliant I feel Becker was.]
So, in a sense, I’m not surprised at the cavalier attitude most staff members have towards people coming into Emergency departments everywhere. Don’t get me wrong. There are some very dedicated and caring medical staff working in ERs doing a mostly thankless job which, I’m sure, can be extremely rewarding at times too but the system is stacked against them and they will, I’m certain, be looking for different work soon if they don’t toe the line. And, of course, as I’ve already noted in a previous post that pain is invisible so ER staff can’t just take your word for it. Not only that, but if you come in really agitated that you’re in extreme pain and need some meds now they may tag you as a troublemaker and make you wait all that much longer for help. There’s a big screen tv in the ER waiting room at the Royal Jubilee Hospital explaining in great detail why you must wait and why. There are signs saying no foul language or threats or whatever will be tolerated. There are security people everywhere dressed just like police. I wonder what they would do if somebody with Turette’s Syndrome came in following a car crash or, as is quite common, some people can’t utter a full sentence without ‘fuck’ in it at least once. These people may just suffer from undeveloped communicative skills but they are probably not dangerous. The message is clear: if you want treatment here you had better stay calm, cool, and collected. Of course, precautions must be taken, but I’m not sure that blanket prohibitions are the way to do it.
Pain, in our culture, is associated with weakness and most people are loathe to talk about it even to the point of not seeing a doctor because they’re embarrassed about the location of their pain or don’t want to admit weakness. Weakness of any kind is just not acceptable. Do you see any weak superheroes in the movies? Well, some of them show some slight or passing weaknesses but they always triumph over them in the glorious light of their super strength. That’s in the movies. In Diehard movies the hero falls off of an eighteen storey building onto the top of a moving van below, rolls of of that onto the sidewalk where he encounters villains walking towards him shooting up a storm with their AR-15s (or whatever), gets hit, falls through the open door of a bar, sidles up to the bartender and asks for a scotch on the rocks. The young, gorgeous, female bartender gives him his drink and comments on the two gaping bullet wounds on his shoulder. He respond in true superhero in training fashion: “These, nah, just flesh wounds.”
Real heroes are immune to pain it seems so if you really want to be a superhero, boys and girls, don’t complain about pain!
Pain doesn’t kill. It’s a sign that something organic is out of whack and needs attention. Failure to attend to pain often results in dire consequences for the patient but any complaint of pain is not treated initially by medical staff as an organic issue, but rather as a moral one. We are all assumed to be moral degenerates unless proven otherwise by the cognoscenti. Of course that’s not true in every case, but the underlying assumptions are always there. Overlying all of this too is the assumption that there is an acceptable amount of demonstration allowed with different levels of injury. So, for a broken leg, some amount of whimpering is allowed, and for the pain I went in with some moaning and groaning is okay, but only when there’s movement happening otherwise sitting quietly is what’s expected. In any case they have a scale of acceptable pain demonstration. Don’t mess up their expectations and assumptions. But as I said, our reaction to pain culturally is really screwed up so you’d have to think that in an ER that would be doubly evident. It’s not right but that’s the way it is. Is there anything we can do about it? Maybe, but it’s complicated and requires a lot of knowledge and challenges to authority. Authority does not like being challenged. That itself is a challenge since authority has all the lawyers it wants to line up against you, often using your money. But lets poke the beast a little and see if it demonstrate any signs of weakness or pain.
I’m not dead yet, and I’m coming for you, VIHA, and related government departments and agencies. You’re trying to get rid of pathology services entirely in the North Island and that’s a travesty. Some of you in the business may need to retake your Hippocratic oath. More on this later. I need to do more research to know exactly what the situation is, but when I’m ready you’ll know about it.
So, for now, I’ve seen my oncologist, my kidney specialist, my pathologist and now I need to have my beer specialist on my team. I won’t be going out to see him anytime soon, but I heard he might just deliver. Damn, there’s so much more to say!
One of my previous posts about disability and people in wheelchairs. It might be of interest after reading this post.
Maybe tomorrow I’ll be in less pain. I have a lot to write about my recent experience with pain but my neck pain is so bad right now I can’t look down and can barely move it from side to side. Tomorrow, I’ll try again. The docs found in a recent CT scan that I have severe disk degeneration in my neck. ‘They’ say that’s what causing my extreme pain at the moment and the pain cannot be attenuated by pain killers, including hydromorphone. I guess that cancer wasn’t enough for me.
In the meantime, as a bit of a primer, I’m reposting a blog post from earlier this year on the subject of pain.
The Conundrum of Pain…and Suffering: Part 1.
I’ve been thinking about writing this piece for a long time. It’s only now that I figured out how I wanted to organize my narrative. It’s complicated because there are so many aspects and approaches to both pain and suffering. The medical profession (and the medical ‘industry’) has its clear claim on the alleviation of pain and suffering. Philosophers and psychologists have also long been interested in the topic. Sociologists too. I won’t be quoting any sources this time. I will leave that for subsequent posts where I deal with specific scholarly and popular approaches to pain and suffering. To start, I want to suggest why I find pain and suffering of interesting.
Pain is not something that can be empirically determined. It cannot be objectively measured as far as I know. If you know otherwise, please let me know. That’s why doctors (MDs, that is) sometimes ask you: “On a scale of 1 to 10, how bad is your pain right now?” You answer: “Gee, I don’t know.” And you just throw out a number because it’s such a hard question to answer. You don’t want to say 2 because then what the hell are they doing in their office? You don’t want to say 10 unless you’re writhing in pain on the floor by the examination table. A 7 is usually good for attracting attention without getting ‘the look’. Still, your doctor may be wary.
You can look at anyone, I don’t care whether they have just been badly damaged in a car crash, they have arthritis, psoriasis, lumbago (don’t you just love that word?), and/or gout. You can impute that they’re in pain, but it’s not visible. Pain is not visible. You cannot see pain. It hides in the crevices, nooks and crannies of your body but nobody can see it so how do we know it’s really there? We may see a person with a massive slashing knife wound to the chest and we assume that person is in pain, but we never see the pain so we don’t have any way of determining its intensity or how much shock or other factors have mitigated or attenuated it.
Recently we (Carolyn and I) spent some time in a hospital emergency department because Carolyn needed an emergency appendectomy. All is much better now, but it was obvious that the medical staff was at a loss the first time we went to emerg (that’s what they call it, you know) to figure out what the cause of Carolyn’s pain might be. They may have even wondered whether or not her pain was psychosomatic. They poked and prodded her, took blood and did a CT scan. Nothing of significance was found. I don’t know what the staff thought at the time. They told her she was a conundrum and looked great on paper. In any case, we were sent home with instructions to take antibiotics, pain killers, etc. When over the next few days the pain got worse for Carolyn we went back to emerg after Carolyn was told by her family doctor that she had a classic case of appendicitis. After a few more hours sitting in waiting rooms and getting more tests including a second CT scan, it was determined that indeed, Carolyn had acute appendicitis (which we subsequently found out was evident on the first CT scan). Time for surgery for a ruptured appendix. This entire scenario was upsetting and did not need to happen. Surgery after our first visit would have been routine and we probably would have come home the same night. As it stood, Carolyn spent two days in the hospital recovering. Now, this was all nasty and everything, but I have questions about the presence of pain as Carolyn described it and the CT scan that showed an inflamed appendix. Did they operate because of the pain or because of the CT scan? The CT scan confirmed that there was an organic problem and the assumption that Carolyn was in pain may or may not have factored into the decision to operate. I’m not sure how that works.
Pain is not something that is determined objectively so how are medical personnel to know whether a person is in pain or is faking it? There are people out there who crave attention (or drugs) and will fake medical symptoms to get it. There are people who have what’s called indeterminate illnesses or diseases of indeterminate etiology like fibromyalgia. Some medical doctors and others associated with medicine still don’t believe that fibromyalgia is a thing. They argue that if only you’d relax, your pain would go away…that’s if you ever really had pain…wink, wink, nudge, nudge. It’s a tough call because pain is not visible. People may be grimacing and walking abnormally, and we assume they’re in pain, but we just don’t know for sure. There is probably more attention given to determining the etiology of pain in regular and emergency medicine than anything else. Guesswork has to play a major role along with targeted questioning. “Does it hurt here? No. Here? No. Then what about here? Okay, here then! Well then, we’ll just peel you off the ceiling now and figure out what to do for you. You will definitely need some painkilling meds. Get that IV hooked up. It’s certainly true that pain alone cannot trigger surgery. Just because I tell a doctor I’m in pain, that doesn’t justify her throwing me straight into the operating room. Subjective reports of pain must be supported by evidence of organic abnormality, or is it the other way around?
Killing pain is huge business. We don’t seem to like pain a lot unless we have a personality disorder and we’re masochistic. Big Pharma’s bread and butter is in killing pain. Opioids are huge business. They are used medically to mitigate physical pain symptoms, but they are also used on the street to deal with ‘psychic’ pain. [This is a topic for another blog post.]
Strangely enough, we often put ourselves through a lot of pain and suffering to accomplish a task that we’ve imposed on ourselves like running a marathon. Why run a marathon only to feel intense pain during and afterwards? What drives us to doing this kind of thing? [This is a topic for yet another blog post.]
Then, there are people, a very small minority, who cannot feel physical pain at all. They can put their hand on a hot stove element and not know that they are in trouble until they smell flesh burning. That’s not a scenario that appeals to me at all. In view of this it’s common to consider that pain has benefits in an evolutionary sense. It’s probably a damn good thing that we do feel pain. Too bad our pain is not obvious to others in an objective way. It would make life a lot less painful for a lot of us.
[Stay tuned. I learned today about myeloma and pain. I also learned that my kidney is fine and I can have beer and wine again.]
Alright, I have a confession to make. I’m not always the most reasonable person around. The photo above is of our fifty-year-old, sixteen foot “Huron” canoe outfitted with outriggers, a mast and sail, along with a deep-cycle battery and an electric motor, and paddles of course. First off, it’s a canoe, not a sailboat, but it did sail very well in moderate to somewhat higher winds. It’s tied here to a stump on Buttle Lake near Ralph River Provincial Campground where we recently spent a few days. The lake was relatively calm. We probably paddled and used the motor to get to this spot not far away from the campground.
On another day, however, we went out in relative calm and while we were out there, the wind blew up. It often does in the afternoons on Buttle Lake. We sailed very quickly to a spot down the lake called Auger Point, a three-kilometre run. Getting back from there was anything but pleasant. We should have known better. Happily, we had the motor that I cranked to full power but even with that we had to paddle at ramming speed to get back to the river mouth where we kept the boat tied up, maybe a kilometre to our camp site. That was one tiring run home. It would have been different had we been able to sail closer to the wind, but with the sail we had and the lack of a leeboard, we were in for a rough upwind fight. Carolyn and I are experienced canoeists and at no time did I feel like we were in trouble, but paddling as hard as we could was feasible even ten years ago, not so much now that I’m 72 and Carolyn is handicapped by arthritis in her hands. Still, we are strong paddlers and we made it without swearing and berating ourselves too much. Now, having done this once and also having promised ourselves to never do it again, what do we do? We go out there again on another day and get caught in the snottiest wind and wave conditions I think I’ve ever seen on the lake. What can I say? Again, we went out on a day that promised to be benign so we headed up the lake looking for a nice place to swim. We paddled down to a bay maybe four kilometers from the campground but there was someone on the beach playing music and fishing from shore. So, we headed down and across the lake to a bay still some distance from the campground where we knew we could skinny dip. As we enjoyed the beautiful lake water and the most enjoyable swim, the lake decided to turn against us, and the wind started blowing strongly from the north. We set out with the motor at half throttle, but we soon had to up that to full throttle and full on paddle to boot. Well, we’ve had some situations in the past where we paddled as hard as we could against a wind without making much headway at all. But we were young then and had much more energy and stamina than we do now. Coming around the point close to the campground we were hit with two-foot chop. That was fine as long as we were able to paddle directly into the wind, but that was not possible as we rounded the point moving east towards the campground. We were abreast to the wind, paddling as hard as we could with the assistance of the motor, and we were being beaten hard by the waves to the point where we started taking on water from the port side. Sensing that we probably couldn’t make it back to the river’s mouth where we would have preferred to leave the boat, we turned the boat downwind and took her into shore on a muddy, unpleasant part of the lakeshore, but still within easy walking distance to our campsite. That’s where she stayed overnight.
The next morning, we took her around to the river’s mouth. We were exhausted, especially me, and I hurt everywhere. Silly us. After that episode, we got reasonable and didn’t do it again. Actually, we got our best swim of our stay on Buttle Lake a couple of days later with no trouble.
The family joined us last Thursday and that was great, but I felt a pain in my right side and shoulder that was getting worse and worse. There’s no doubt in my mind that fighting the extreme winds on Buttle not once but twice contributed significantly to my injury. I was definitely injured. The pain got so bad (pushing 9.5 out of 10) that I was very relieved to know that I had some T3s in my toiletry bag. I took two and felt hardly any relief. Later, I took two more along with some CBD and THC (I have a prescription for them). I managed to sleep fitfully although some people might suggest I was not sleeping as much as in an altered state of mind. The next day the pain had not attenuated at all, and we had to leave the campsite and head home. I couldn’t help pack up at all and my son-in-law was conscripted to drive the truck home towing our old eighteen-foot Holidaire trailer. I could barely sit still on the way home, having to shift my weight often to try to lessen the pain. The drive home was uneventful, but I still hurt, easily pushing 6 out of 10.
After being home for a bit and still at the end of my rope trying to deal with pain that prevented me from even taking a deep breath, I took two ibuprophen, went to bed for an hour or so and got up feeling fine. A miraculous recovery! I would have taken ibuprophen a lot earlier, but I was counselled in 2002 after my left kidney was removed because of cancer that I should avoid anti-inflammatory meds. I didn’t take any until this past weekend and just took two more a few minutes ago. The meds are still keeping the pain at bay, but I’m loathe to keep taking anti-inflammatory meds like ibuprophen because they are hard on the kidneys. So, tomorrow I call my doctor and make an appointment to see if there are any alternatives to ibuprophen I can take that might help mitigate acute pain. I’m used to chronic pain, but the acute pain brought on by the foolishness in our canoe was untouched by acetaminophen, even with codeine, and even supplemented with CBD and THC. My problem seemed to me clearly one of muscular inflammation. It’s clear that I need a solution to deal with acute pain because I can’t promise to always be reasonable in the future. My family was extremely supportive, and I love it for that, but I feel that I need to pull my own weight too. I will not always have my family there to support me if I get into unreasonable trouble again. I need good meds too!
Human beings kill. We kill plants and animals at an incredible rate and transform their basic life elements into ourselves when we eat them. We cannot do otherwise. We must ingest other organisms to survive. We are generally omnivorous. That means we will shove anything and everything down our throats even if now and again we choke on something. So, we kill for food. We also kill for fur, bones, scientific research and just for fun. We seem to enjoy driving lead into other animals and into each other. We have institutions that encourage it, thousands of them. The market is one of the most important ones but the military is close behind as is factory farming both on land and water.
For this blog post, however, I want to focus on one historical incidence of our obsession with killing other animals, and it’s on beaver that I focus my attention here. This post is about our obsession with killing beaver leading to the creation of Canada.
I’ve already written about how the fur trade was initially (in the 16th Century) incidental to the fishery on the Grand Banks and the Gulf of St. Lawrence. From there, and moving into the 17th Century, the fur trade moved inland. Samuel de Champlain first arrived in the St. Lawrence River in 1603 and in the next couple of decades travelled up the Ottawa River, along a trade route that had existed long before contact, to the Mattawa, Lake Nippising, the French River and on to Georgian Bay, Lake Huron, and Lake Superior. In 1968, Parks Canada published a book by Eric W. Morse called Fur Trade Canoe Routes of Canada/Then and Now. With an introduction by Pierre Elliot Trudeau, who canoed with Morse on occasion, the book presents a detailed first hand exploration of historical fur trade routes and their conditions as of the publication of Morse’s book in 1968. The current landscape barely resembles the one extant when Champlain first explored it in the first half of the 17th Century. It seems we just couldn’t leave well enough alone. We killed off most of the beaver whose dams mitigated flooding and erosion and replaced them with concrete dams and culverts. What could go wrong? Ask Sudbury. It just declared a climate emergency. It sits at the epicentre of the historic beaver kill off.
Morse’s book clearly shows how the fur trade routes originating in the St. Lawrence essentially followed the southern edge of the Canadian Shield all the way to Lake Athabasca via Lake Superior, Rainy Lake, Lake of the Woods, Lake Winnipeg, the North Saskatchewan River, and winding it’s way into the Mackenzie River drainage system through La Loche in what is now northern Saskatchewan. In a sense, a shorter route to the interior was via Hudson’s Bay and it’s drainage system which included Lake Winnipeg, but which followed a number of routes inland depending on the time of year and the conditions at the time. The fur trade necessarily followed the geography of the rivers, lakes, and portages that would lead to the quickest and most efficient route to the money embedded in beaver fur. The further away from salt water the beaver had to be hunted because of their depletion along the established routes the more the trade cost in terms of infrastructure and human power. For the first hundred years until at least the 1650s, Europeans had not set foot in the interior as traders. Indigenous middlemen such as the Algonquin, the Huron and later the Odawa and others west of the Great Lakes, including the Chippewa, Ojibwa, Potawatomi and further west, the Dakota Sioux, the Assiniboine and the Cree. In the north, the Chipewyan were dominant. To the west of them the Strange, the Sikani and the Carrier among others east of the Rockies. The Tlingit provided important trade routes to the West Coast as did the Tahltan who were connected to the coast along the Stikine River, and other groups.
Every Indigenous group in what is now Canada coveted European trade goods the moment they first encountered them and did whatever it needed to do to get them including waging war with their neighbours or competitors wherever they might live. For instance, the Iroquois (as we know the Haudenosaunee) terrorized the Montagnais and other groups who trapped beaver and wished to trade with the Europeans along the St. Lawrence and down the Richelieu River to Lac Champlain and beyond. By 1650, the Iroquois (mostly the Mohawk) had routed the Huron and broken up their Georgian Bay trading empire. The Wendat (Huron) had earlier displaced the Algonquin. Once they became dependent on European trade goods, Indigenous peoples no longer had fetters in their hunt for beaver. They participated wholeheartedly in the industrial pursuit of beaver fur. Indigenous peoples were the workforce for the fur trade and were thus not deliberately eliminated. The Americans, in contrast, worked to systematically eradicate indigenous populations south of the St. Lawrence and the Great Lakes all the way to the Gulf of Mexico because they were in the way of agricultural settlement moving west at an increasingly rapid rate. They did not succeed entirely but there is little left of pre-contact indigenous culture. Of course it’s true that there is very little left of European culture of the 15th Century either.
To follow the settlement of the west in the early 1870 with the creation of Manitoba and British Columbia, with Alberta and Saskatchewan in 1905 is to know that the area north of the 49th Parallel was to remain tied to the British Empire as a part of Canada. The Americans realized early that they could advantageously trade with the Northwest Company to bring furs through Michilimackinac. John Jacob Astor of the American Fur Company, the wealthiest American of the time arranged a deal where his company, the Michilimackinac Company, and the Northwest Company agreed to mutually respect ‘their’ territories. Astor was an astute businessman and negotiator. His strengths as a trader lay on the Pacific Coast and in the Lake Michigan area and he was more than willing to leave the north to the British (for a price). Ultimately the trade in beaver fur would be the base of his wealth, but it would not remain so. Astor made most of his wealth in New York real estate after the signs of the demise of the fur trade were too clear to ignore. Harold Innis writes:
“The northern half of North American remained British because of the importance of fur as as staple product. The continent of North America became divided into three areas: (1) to the north in what is now the Dominion of Canada producing for, (2) to the south in what were during the Civil War the secession states producing cotton, and (3) in the center the widely diversified economic territory including the Now England states and the coal and iron areas of the middle west demanding raw materials and a market. The staple-producing areas were closely dependent on industrial Europe, especially Great Britain. The fur-producing area was destined to remain British…
The Northwest Company and its successor the Hudson’s Bay Company established a centralized organization that covered the northern half of North America from the Atlantic to the Pacific…It is no mere accident that the present Dominion coincides roughly with the fur-trading areas of northern North America…The Northwest Company was the forerunner of the present confederation.” ( from The Fur Trade in Canada, Yale University Press, New Haven, 1930, page 396)
From this perspective, the true Fathers of Confederation are Alexander Mackenzie, David Thompson and Simon Fraser of the Northwest Company rather than John A. Macdonald and Etienne Cartier.